Key Points
General points to uphold in the approach to the chest radiograph, before reviewing the film for cardiovascular detail, include the following:
- ▪
Review the indication for the radiograph
- ▪
Avoid cases of mistaken identity. Confirm the identity of the patient.
- ▪
The accuracy of the conclusions is based on the quality of the radiograph.
- ▪
Was the inspiration adequate?
- ▪
Was the patient well centered? If the patient’s body was significantly rotated, be wary of interpreting mediastinal contours that would be projected differently.
- ▪
Was the penetration/exposure optimal for the purposes of examining the heart? If it was not optimal, adjust the windowing as needed to review the heart, devices within the heart, the aorta, and the lungs.
- ▪
- ▪
When possible, review serial chest radiographs.
Indications for Chest Radiography
Chest radiography is indicated for all patients admitted to hospital because of a cardiovascular diagnosis and can arguably be said to be indicated at the initial assessment of all outpatients evaluated for suspected cardiovascular diagnoses. The ability of the chest radiograph to estimate heart size, image pulmonary vascular and aortic findings, lung parenchymal and pleural disease, and chest wall pathology contributes to the management of cardiovascular disease patients with many diagnoses such as the following:
- □
Coronary artery disease
- □
Congestive heart failure
- □
Valvular heart diseases
- □
Prosthetic heart valves
- □
Myopathic diseases
- □
Pericardial diseases
- □
Aortic diseases
- □
Hypertension
- □
Congenital heart and vascular diseases
- □
Chest pain syndromes
- □
Post–cardiovascular surgery
- □
Post–thoracic aortic endografting
- □
Suspected cardiovascular trauma
Additional reasons to perform chest radiography at initial assessment include the relatively high frequency of pulmonary disease in the adult cardiovascular patient and the ability of the chest radiograph to image some of these forms of pathology. Adverse change in clinical status and need to assess treatment effect should also prompt chest radiography. Hence, a liberal strategy for the use of chest radiography is appropriate because, in general, the modality is often underused; thus proficiency with its use and interpretation (outside of radiology) is often suboptimal.
Review of the indication for imaging helps establish an approach and awareness of various possible complications or associations.
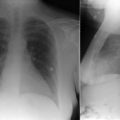
Standard chest radiography includes a frontal (posteroanterior [PA]) radiograph and a lateral radiograph. The frontal radiograph is taken with the patient’s back toward the incident x-rays to minimize the amplification of the size of the heart shadow. The two radiographs are complementary and confirmatory to each other. To have PA and lateral radiographs taken, the patient must be able to stand or lean against a screen with his or her arms abducted. PA and lateral radiographs are taken in radiology facilities. It is not possible to routinely take high-quality PA and lateral radiographs with portable x-ray equipment. The quality and amount of information offered by PA and lateral radiographs make them more useful than portable radiographs, and they are far and away the first choice whenever possible. Therefore chest radiography should include PA and lateral radiographs, except for critically ill, unstable, or suspected unstable patients.
Portable radiographs are taken with the patient sitting in bed (preferable) or lying in bed (often the only option for critically ill patients) with the radiograph plate behind the patient’s back. The x-ray–generating equipment is facing the patient, either at the foot of the bed or over the bed; hence, the incident x-ray beams enter the patient in an anteroposterior (AP) fashion. Consequently, the size of the heart shadow is exaggerated. Sicker patients who have portable AP radiographs, rather than standard PA and lateral radiographs, are often unable to take a deep breath or sit erect (or even upright), which alters many factors such as alignment/projection and the lung volume/ratio of the heart size to the chest width. Hence, the technical quality of portable x-rays is usually far lower than that of standard radiographs for a combination of reasons. Nonetheless, portable chest radiographs are extremely useful for verification of chest tube and catheter placement and for following the clinical course of pulmonary edema, pulmonary parenchymal diseases, and pleural effusions.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


