Abstract
For oncologic FDG PET/CT scans, the patient is in the fasted state and the myocardium has variable utilization of glucose versus other sources of energy for metabolism. This results in a highly variable appearance of the myocardium on PET/CT, ranging from no apparent FDG-uptake to very prominent FDG-uptake. Focal areas of FDG-avidity in the heart may correspond with physiologic structures, such as the papillary muscles or lipomatous hypertrophy of the intra-atrial septum. Suspicious FDG-avid foci in the heart may be further evaluated using echocardiography or cardiac MR.
Keywords
FDG, PET/CT, heart, myocardium, papillary muscle, lipomatous hypertrophy of the intra-atrial septum, cardiac sarcoma
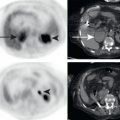
With a recent glucose load, the myocardium uses glucose as its primary energy source. When fasting, the myocardium switches to using fatty acids rather than glucose. The longer the fast, the more likely the myocardium will be using fatty acids. This is why for a cardiac 18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG PET/CT), when we want to evaluate cardiac ischemia and infarcts, the patient is given a glucose load prior to the PET/CT, to make the myocardium take up glucose and FDG. For an oncologic FDG PET/CT, the patient fasts at least 4 hours. This decreases glucose and FDG uptake in skeletal muscle. This also has the effect of decreasing glucose and FDG uptake in the myocardium. For most FDG PET/CT studies with a 4- to 6-hour fast, it is difficult to predict how much physiologic FDG uptake will be seen in the myocardium. This results in a highly variable appearance of the myocardium on oncologic FDG PET/CT. There may be no apparent FDG uptake, uptake in part or all of the left ventricle, even uptake in right ventricle or atria ( Fig. 10.1 ). It is important not to mistake areas of no FDG uptake as infarctions on oncologic FDG PET/CT studies. Indeed, on an oncologic FDG PET/CT, focal areas of FDG photopenia are often physiologic, rather than infarcts or ischemia (see Fig. 10.1B ).

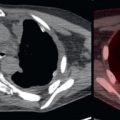
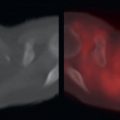
Focal areas of FDG avidity in the heart may correspond with physiologic structures. One or more of the left ventricular papillary muscles may be focally FDG avid and are located in predictable locations ( Fig. 10.2 ). The intraatrial septum may undergo lipomatous hypertrophy, and this may be focally FDG avid ( Fig. 10.3 ).