Presentation and Presenting Images
A 61-year-old female presents for screening mammography.
27.2 Key Images
27.2.1 Breast Tissue Density
There are scattered areas of fibroglandular density.
27.2.2 Imaging Findings
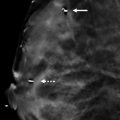
In the upper outer quadrant of the left breast at the 2 o’clock location in the posterior depth, there is a 1.5-cm irregular high-density mass ( ▶ Fig. 27.3 and ▶ Fig. 27.4). The right mammogram was negative (not shown).
27.3 BI-RADS Classification and Action
Category 0: Mammography: Incomplete. Need additional imaging evaluation and/or prior mammograms for comparison.
27.4 Diagnostic Images
( ▶ Fig. 27.5, ▶ Fig. 27.6, ▶ Fig. 27.7, ▶ Fig. 27.8, ▶ Fig. 27.9)
27.4.1 Imaging Findings
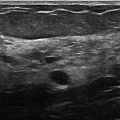
The diagnostic imaging demonstrates a persistent 1.5-cm irregular high-density mass with indistinct margins at the 2 o’clock location in the posterior depth ( ▶ Fig. 27.5, ▶ Fig. 27.6, and ▶ Fig. 27.7). The targeted ultrasound reveals a 1.0 × 0.7 × 1.3 cm irregular hypoechoic mass with indistinct margins and posterior acoustic shadowing at 2 o’clock position, 3 cm from the nipple ( ▶ Fig. 27.8). There is mild vascularity adjacent to the mass but not internally ( ▶ Fig. 27.9). The ispilateral axillary lymph nodes were normal (not shown).
27.5 BI-RADS Classification and Action
Category 4C: High suspicion for malignancy
27.6 Differential Diagnosis
Invasive ductal carcinoma (IDC): Core needle biopsy revealed grade 2 IDC with intermediate grade ductal carcinoma in situ (DCIS). The imaging features would support the diagnosis of any invasive carcinoma.
Normal breast tissue: This mass should not be interpreted as normal breast tissue. The conventional mammogram and DBT both support that this is a mass as defined by its convex margins. A biopsy revealing normal breast tissue would be considered discordant with these findings.
Fibroadenoma: This mass has an irregular shape with indistinct margins both mammographically and on ultrasound. These imaging findings would not support a benign diagnosis.
27.7 Essential Facts
Invasive ductal carcinoma is the most common invasive breast cancer (65–75% of cases).
Most invasive ductal carcinomas are sporadic; only about 10% of cancers are attributable to genetics.
The incidence of breast cancer increases with age.
Over half of invasive ductal carcinomas are clinically occult and detected by imaging.
There is a better prognosis for breast cancers identified at screening compared to interval cancers (cancers detected between screening examinations). This is despite accounting for positive lymph nodes, tumor size, patient age, hormone receptor status, and histological grade. The method of detection (screening or interval) may not have independent prognostic utility, but only that screening leads to earlier detection of cancers.
27.8 Management and Digital Breast Tomosynthesis Principles
In several studies, digital breast tomosynthesis (DBT) has been shown to decrease the recall rate for further imaging evaluation.
DBT has shown improved sensitivity and specificity for cancer detection across all breast tissue densities.
DBT, due to its ability to reduce anatomical noise within a given slice, especially in dense breast tissue, can better assess the size of a tumor and its imaging characteristics. This leads to improved accuracy of diagnosis.
When full-field digital mammography (FFDM) and DBT are performed in combination, , there is an approximate doubling of the radiation dose for FFDM alone.
27.9 Further Reading
[1] Förnvik D, Zackrisson S, Ljungberg O, et al. Breast tomosynthesis: Accuracy of tumor measurement compared with digital mammography and ultrasonography. Acta Radiol. 2010; 51(3): 240‐247 PubMed
[2] Shen Y, Yang Y, Inoue LY, Munsell MF, Miller AB, Berry DA. Role of detection method in predicting breast cancer survival: analysis of randomized screening trials. J Natl Cancer Inst. 2005; 97(16): 1195‐1203 PubMed

Fig. 27.1 Left craniocaudal (LCC) mammogram.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


