Hip Ultrasound

Clinical photograph shows the patient and probe position for examination of the anterior hip recess. The patient lies supine with the hip extended. Internal or external rotation of the hip during scanning of the anterior hip structures can be helpful.

Oblique longitudinal US shows the anterior recess  of the hip joint anterior to the neck
of the hip joint anterior to the neck  and head
and head  of the proximal femur.
of the proximal femur.

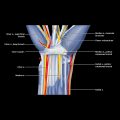
Longitudinal US shows the capsular attachment  to the rim of the acetabulum. The labrum
to the rim of the acetabulum. The labrum  is hypoechoic due to anisotropy. The femoral head of articular cartilage
is hypoechoic due to anisotropy. The femoral head of articular cartilage  is clearly seen. Part of the rectus femoris tendon attachment
is clearly seen. Part of the rectus femoris tendon attachment  is visible.
is visible.

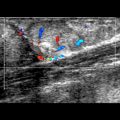
Transverse US at the level of the femoral head shows the close relationship between the femoral head  , the acetabulum
, the acetabulum  , and the iliopsoas tendon
, and the iliopsoas tendon  and muscle
and muscle  .
.
GENERAL CONSIDERATIONS
Clinical Indications for Hip US
TECHNIQUE: ANTERIOR HIP
Patient Position
Specifically Examine
 First identify rounded cortex of femoral shaft in midthigh and trace in transverse plane proximally
First identify rounded cortex of femoral shaft in midthigh and trace in transverse plane proximally
 At intertrochanteric region, where bone contour is seen to widen, rotate medial aspect of transducer upward to align longitudinally along femoral neck
At intertrochanteric region, where bone contour is seen to widen, rotate medial aspect of transducer upward to align longitudinally along femoral neck
 Anterior joint capsule is seen extending from acetabulum to intertrochanteric line; superficial capsular fibers extend over proximal femoral shaft, while deep fibers reflect backward to head/neck junction
Anterior joint capsule is seen extending from acetabulum to intertrochanteric line; superficial capsular fibers extend over proximal femoral shaft, while deep fibers reflect backward to head/neck junction
 Each collagenous layer is seen as 2-4 mm thick echogenic band, while inner synovium is too thin to be seen
Each collagenous layer is seen as 2-4 mm thick echogenic band, while inner synovium is too thin to be seen
 Normal thickness of anterior recess from outer margin capsule to bone is 6-8 mm
Normal thickness of anterior recess from outer margin capsule to bone is 6-8 mm
 If no effusion, both capsular layers are opposed ± thin intervening hypoechoic line (stripe sign) representing anterior hip recess
If no effusion, both capsular layers are opposed ± thin intervening hypoechoic line (stripe sign) representing anterior hip recess
 Normal contour of anterior capsule is concave or flat rather than convex in outline
Normal contour of anterior capsule is concave or flat rather than convex in outline
 Transducer in oblique transverse plane just proximal to hip joint
Transducer in oblique transverse plane just proximal to hip joint
 Patient is asked to reproduce symptoms or else move hip from flexion-abduction to external rotation to neutral position during real-time scanning in transverse plane
Patient is asked to reproduce symptoms or else move hip from flexion-abduction to external rotation to neutral position during real-time scanning in transverse plane
 Normally, iliopsoas tendon and muscle will move laterally in smooth clockwise fashion
Normally, iliopsoas tendon and muscle will move laterally in smooth clockwise fashion
 Snap usually produced and felt as sudden flip of iliopsoas tendon around iliacus muscle
Snap usually produced and felt as sudden flip of iliopsoas tendon around iliacus muscle
 Asymptomatic snapping is quite common finding on testing normal subjects
Asymptomatic snapping is quite common finding on testing normal subjects
 On transverse and longitudinal scanning proximal to hip joint, characteristic rectus femoris tendon with direct and indirect heads
On transverse and longitudinal scanning proximal to hip joint, characteristic rectus femoris tendon with direct and indirect heads
 Evaluate rectus femoris tendon from both medial and lateral sides to see both direct and indirect tendons
Evaluate rectus femoris tendon from both medial and lateral sides to see both direct and indirect tendons
 More distally, within proximal rectus femoris muscle, indirect tendon → central aponeurosis, while direct tendon → superficial aponeurosis
More distally, within proximal rectus femoris muscle, indirect tendon → central aponeurosis, while direct tendon → superficial aponeurosis
 Rectus femoris tendon is C-shaped
Rectus femoris tendon is C-shaped
 Observe inguinal ligament, sartorius medially, and tensor fascia lata muscle laterally
Observe inguinal ligament, sartorius medially, and tensor fascia lata muscle laterally
 On transverse scanning, proximal ends of these muscles can have pseudothyroid appearance
On transverse scanning, proximal ends of these muscles can have pseudothyroid appearance
 On longitudinal scanning, short tendons and attachments of these muscles are best seen
On longitudinal scanning, short tendons and attachments of these muscles are best seen
 Observe lateral femoral cutaneous nerve deep to lateral aspect of inguinal ligament
Observe lateral femoral cutaneous nerve deep to lateral aspect of inguinal ligament
 Nerve moves from medial to lateral over iliacus, then over sartorius to run between sartorius and tensor fascia lata
Nerve moves from medial to lateral over iliacus, then over sartorius to run between sartorius and tensor fascia lata
 Sartorius muscle passes distally over femoral neurovascular bundle
Sartorius muscle passes distally over femoral neurovascular bundle