Hormone Effects
Eva C. Gombos, MD
Terminology
Definitions
Hormone effects: Enhancement and morphological changes induced by differences in hormonal status
Hormone replacement therapy (HRT): Exogenous hormone administration in postmenopausal patients
Selective estrogen receptor modulators (SERMs)
Selectively inhibit or stimulate estrogen-like action in various tissues (distinguished from pure receptor agonists and antagonists)
Anatomy-Based Imaging Issues
Overview
Normal breast tissue enhances post contrast
Estrogens cause parenchymal hyperemia, leading to increased enhancement
Degree and pattern of enhancement vary cyclically in normal premenopausal breast
Maximum enhancement is expected just before and after menstruation (during 1st and 4th weeks)
Menstrual cycle, pregnancy, lactation, and HRT may have profound effects on enhancement of normal tissue
Imaging Recommendations
Document menstrual status (date of last menstruation)
Inquire possibility of pregnancy, lactation, or HRT
Premenopausal women: Ideally during days 7-14 of cycle; may not be feasible
Decreased enhancement in > 50% at repeat MR exams
BI-RADS 3A is used in some facilities to recommend very close interval follow-up (6-8 weeks)
Pregnancy: MR is not advised as Gd-DTPA is known to cross placenta
Ultrasound and mammography are recommended in pregnant patients with suspicious abnormality
Lactation: Extreme enhancement is typical but variable
Minimal Gd-based contrast is secreted into breast milk; ACR guidelines now state it is safe to continue nursing after contrast
Postmenopausal women: Typically parenchymal atrophy and less enhancement
Imaging Pitfalls
Hormonally induced enhancement may mimic disease when focal and rapid; reduced specificity
Hormonally induced enhancement may obscure disease; reduced sensitivity
MR Features
NMLE: Common
Distribution: Diffuse, regional, focal areas
Mass-Like Enhancement
Rarely focal exuberant enhancement may appear mass-like
Enhancement Kinetics
Most common: Low or medium wash-in and persistent delayed kinetics
Correlation with Hormone Therapy
HRT (Combined Estrogen & Progesterone)
Increases risk of breast cancer and thrombosis
Decreases/reverses menopausal parenchymal atrophy
NMLE may occur in at least 30% of patients on HRT
Repeat examination 2-3 months after interruption of HRT can show regression of enhancement
SERMs
All SERMs decrease risk of breast cancer
Tamoxifen has antiestrogen effect on breast
Causes ↓ enhancement and ↓ breast density
Inhibits growth of ER(+) breast cancer
Differential Diagnosis
Normal and Benign
Hormonally responsive breast tissue ± proliferative changes
Fibroadenoma, papilloma, periductal inflammation
Implications and Management
Significance
Certain enhancement patterns may pose differential diagnostic problems
Management must be based on level of suspicion (interval follow-up, biopsy)
Selected References
1. Delille JP et al: Physiologic changes in breast magnetic resonance imaging during the menstrual cycle: perfusion imaging, signal enhancement, and influence of the T1 relaxation time of breast tissue. Breast J. 11(4):236-41, 2005
2. Espinosa LA et al: The lactating breast: contrast-enhanced MR imaging of normal tissue and cancer. Radiology. 237(2):429-36, 2005
3. Pfleiderer SO et al: Changes in magnetic resonance mammography due to hormone replacement therapy. Breast Cancer Res. 6(3):R232-8, 2004
4. Heywang-Köbrunner SH et al: Contrast-enhanced MRI of the breast: accuracy, value, controversies, solutions. Eur J Radiol. 24(2):94-108, 1997
5. Kuhl CK et al: Healthy premenopausal breast parenchyma in dynamic contrast-enhanced MR imaging of the breast: normal contrast medium enhancement and cyclical-phase dependency. Radiology. 203(1):137-44, 1997
6. Müller-Schimpfle M et al: Menstrual cycle and age: influence on parenchymal contrast medium enhancement in MR imaging of the breast. Radiology. 203(1):145-9, 1997
Image Gallery
LACTATION: DIFFUSE BILATERAL ENHANCEMENT
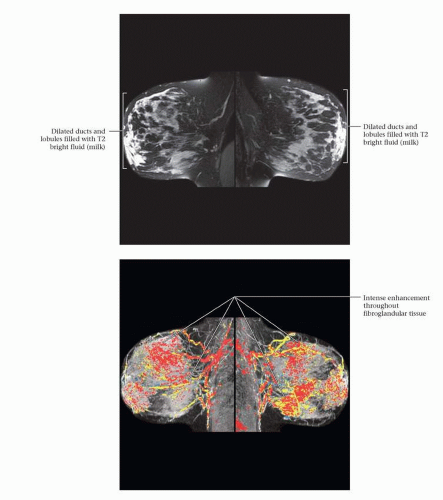 Figure 1 (Top) 42-year-old asymptomatic woman with known BRCA germline mutation. T2W FS images from a surveillance MR performed on this lactating woman show multiple fluid-filled ducts containing high signal due to the breast milk. (Bottom) MIP angiomaps show dense parenchyma and diffuse enhancement throughout the fibroglandular tissue. There is no evidence of an enhancing mass. Both breasts show areas of rapid enhancement and washout. The final assessment was a BI-RADS 2. Intense general enhancement is physiologic and expected in lactating women. Underlying lesions may be obscured by the marked enhancement. |
LACTATION: COMPARISON TO NON-LACTATION
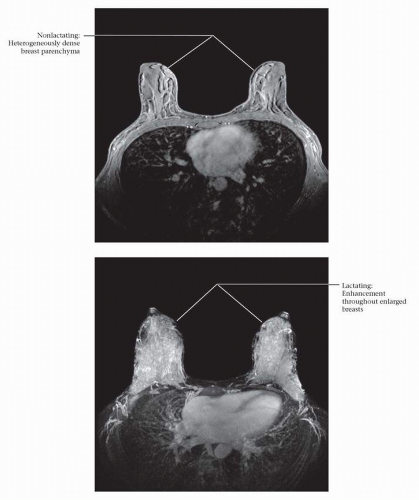 Figure 1 (Top) Asymptomatic 34-year-old woman with a strong family history of breast carcinoma. Heterogeneously dense breast parenchyma is seen bilaterally on baseline surveillance MR. No suspicious enhancing lesion was found. (Bottom) One year later this patient is lactating. Surveillance MR shows exuberant enhancement throughout the enlarged breasts. No focal suspicious lesion is seen, but this pattern of enhancement limits the sensitivity of the examination.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|




