Fig. 7.1
A predominantly cystic pelvic mass containing mural nodularity is detected on contrast-enhanced CT (a) and ultrasound (b). For an accurate diagnosis, the needle must target the solid component of the mass (as shown in c), rather than the fluid component
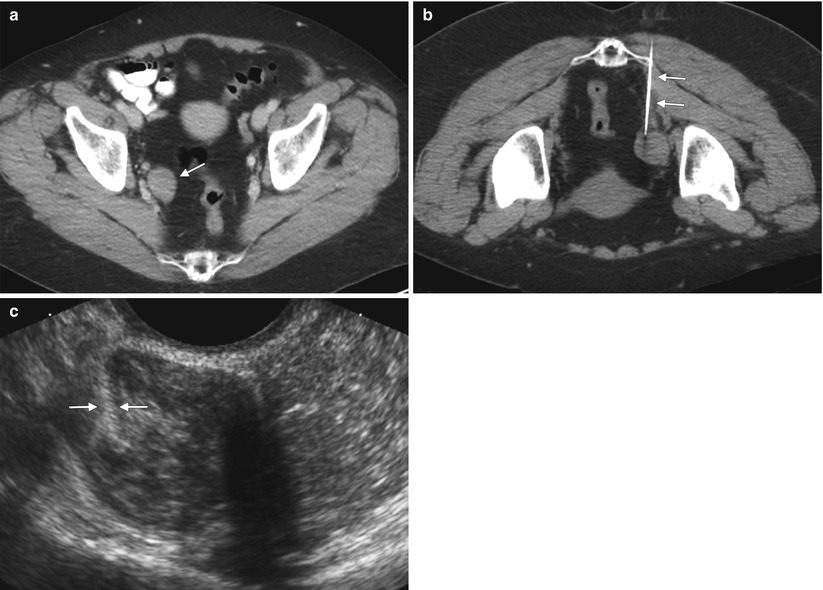
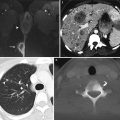
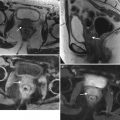
Fig. 7.2
(a) CT scan of a patient with ovarian cancer who previously underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy. This followup CT scan demonstrates a right-sided pelvic mass. (b) In the same patient, CT-guided percutaneous biopsy is performed with the patient in a prone position. The needle is inserted via a posterior approach and is placed into the mass. (c) In the same patient, a transvaginal approach offers a more direct path to the mass. The needle track is seen between the arrows
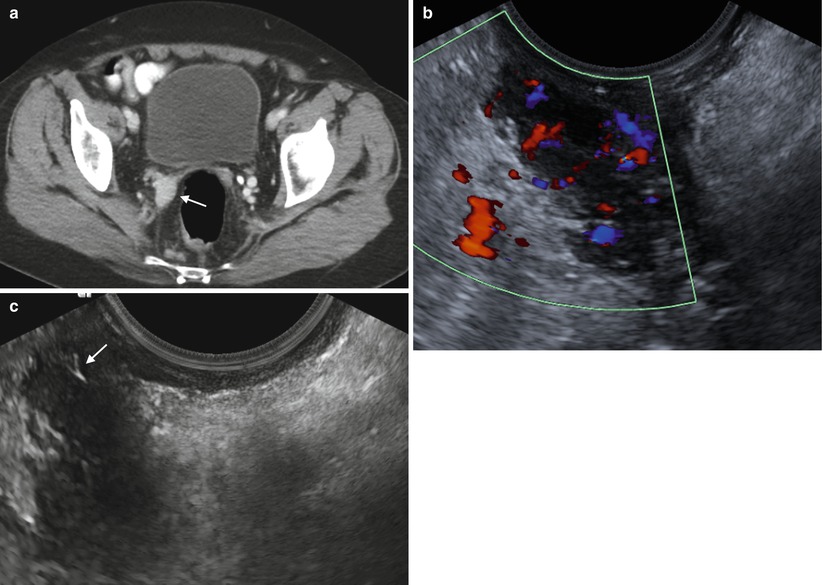
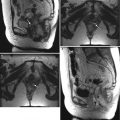
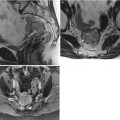
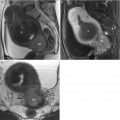
Fig. 7.3
(a) A contrast-enhanced pelvic CT scan shows a solid mass in the vaginal wall. (b) In the same patient, a transvaginal ultrasound shows a hypoechoic mass in the same location. A color Doppler image demonstrates increased internal vascularity. (c) This image of an ultrasound-guided transvaginal biopsy shows the needle inside the mass (arrow), which proved to be non-Hodgkin’s lymphoma. The benefit of the transvaginal approach can be seen by comparing a, b, and c: A transvaginal biopsy avoids passage through the bowel and bladder with an anterior approach, and avoids the sciatic nerve and vessel with a posterior approach
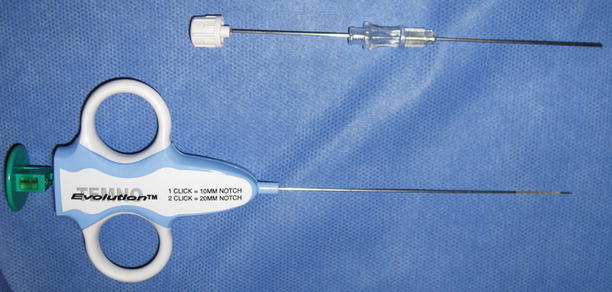
Fig. 7.4
The introducer needle for a core biopsy (top). Once the needle in inserted into the peripheral portion of the target, the stylet (the inner portion of the needle) is withdrawn and the longer needle (with handle, bottom) is inserted into the mass

Fig. 7.5
Ultrasound-guided percutaneous biopsy. The core needle is passed through the needle guide attached to the transducer

Fig. 7.6
A transvaginal transducer, with needle guide and probe cover

Fig. 7.7
After the guide is attached to the transducer, the transducer is inserted into the vagina; then the needle is inserted into the guide
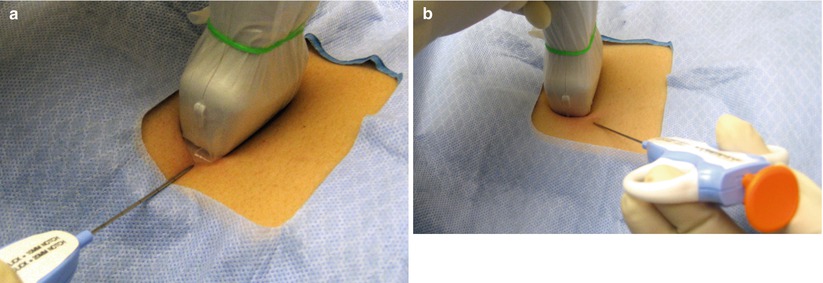
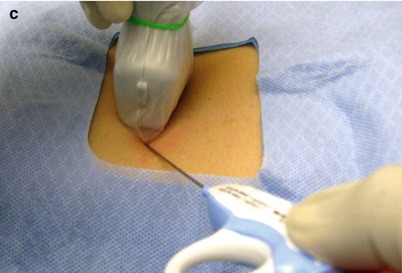
Fig. 7.8
(a) Accurate alignment of the needle with the transducer. (b) Inaccurate alignment: the needle is off center relative to the transducer. (c) Inaccurate alignment: the needle is in the center of the transducer, but angled off to one side
References
1.
Thomas DA, et al. Ultrasound-guided biopsy and drainage of the abdomen and pelvis. In: Rumack CM, Wilson SR, Charboneau JW, et al., editors. Diagnostic ultrasound. 3rd ed. Philadelphia: Elsevier/Mosby; 2005. p. 625–55.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


