Fig. 5.1
A drawing representing the different fracture patterns in pediatric age
A complete fracture is a break that runs the entire width of a bone and it is classified as spiral, transverse, or oblique, depending on the direction of the fracture line [2, 5]. Spiral fractures are usually caused by a rotational, low-velocity force (Fig. 5.2). An intact periosteal hinge enables the orthopedic surgeon to reduce the fracture by reversing the rotational injury [1, 8]. Oblique fractures occur diagonally across the diaphyseal bone and they are unstable; therefore an alignment is necessary (Fig. 5.3). A fracture reduction is attempted by immobilizing the extremity while applying traction [3]. Transverse fractures are determined by a three-point bending force and usually they are easily reduced by using the intact periosteal layer from the concave side of the fracture force (Fig. 5.4). Many of them involve the upper extremities [10, 11] and the clavicle is a typical example (Fig. 5.5). In most cases, fracture of the clavicle concerns the outer third and it is the consequence of a direct blow to the acromion which causes the epiphysis (firmly anchored by the strong acromioclavicular ligaments) to separate from the growth plate and ride upward. Complete mid-shaft clavicular fractures are rare and the medial fragment is usually elevated by the sternocleidomastoid muscle, so that it can be easily displayed on the plain films [12]. The fracture of the distal humerus is more common in children than in adults, but the diagnosis may be difficult owing to the numerous ossification centers. In 60 % of cases, the fracture concerns the supracondylar region and it is crucial to promptly immobilize the arm in order to avoid a neurovascular injury (Fig. 5.6). Lateral condyle and medial epicondyle fractures have a lower incidence (respectively, 15 and 10 %) and the consequence of a delayed diagnosis is severe, since the former has a high potential for nonunion and the latter may be frequently associated with an ulnar nerve injury. The fat pad sign [20, 21] may be the radiological manifestation of an occult fracture in the elbow and it is determined by the distention of a structurally intact joint capsule. Three small masses of fat rest in the radial, coronoid, and olecranon fossae and are enveloped by the fibers of the joint capsule, which separate the fat pads from the synovial lining, making them intracapsular and extrasynovial in location. When there is a joint distention, the anterior fat pad is displaced anteriorly and superiorly and the posterior fat pad is displaced posteriorly and superiorly. The previously invisible posterior fat pad becomes visible on the lateral radiograph of the elbow held in 90° of flexion. However, it must be remembered that not only hemarthrosis or joint effusion due to trauma but also infections, inflammations, or neoplasms can distend the joint capsule and displace the fat pads [21]. Proximal humeral fractures are rare (about 1 % of all the pediatric fractures) and they may be determined by an underlying pathology, such as a bone cyst or a benign tumor (Fig. 5.7). Since the proximal humerus provides for the majority of the longitudinal growth of this bone and has therefore a high remodeling potential, the surgical treatment is not required, and up until the age of 5, a slight degree of fragment angulation is tolerable for a good healing [22, 23]. Forearm fractures are most frequent in children and they are usually associated fractures, meaning that both the radius and the ulna (Figs. 5.4 and 5.5) or the distal radioulnar joint is involved at the same time [11, 23]. In children, the most common forearm fractures concern the distal region of the radius and they are similar to the adult ones both for features and traumatic mechanism (typical are Colles’ fracture and Smith’s fracture). The only difference with elderly patients consists in the treatment, as in children these fractures usually do not involve the joint and the bones have a high remodeling potential so major angulations may be tolerable [24, 25]. Injuries of the proximal region of the radius usually involve the “neck” (Fig. 5.8) because the epiphysis is cartilaginous until the age of 3–6 and it is therefore more resistant to trauma forces. The mechanism is a fall with an open hand on an outstretched and externally rotated arm. Radial fractures may be classified according to the Judet classification [26, 27] which is based on the angulation between the fragments into four grades of severity (Fig. 5.9). A particular kind of associated injury of the radius and ulna is the Monteggia fracture that involves the proximal region of the ulna and is associated with the anterior dislocation of the proximal radius [1, 11]. Fractures of the lower extremities in children are rarer than in adults due to the thick periosteum and the greater content in cartilage that allows a traumatic energy absorption. Pelvic, sacrum, and femoral injuries are all uncommon and they account for 2–8 % of all pediatric fractures. Tibial traumas are slightly more frequent, usually happen in young boys from 8 to 13 years old, and are caused by a fall on an outstretched and internally rotated leg, as in a bicycle fall. The same mechanism in adults may lead to an injury to the anterior “cruciate” ligament while in younger patients may cause the fracture of the tibial spine. Injuries of the tibial shaft are frequent especially when infant begins to walk (from 10 months to 3 years old) and so they are usually called toddler’s fractures (Fig. 5.10). They are often closed and incomplete [4, 11, 28, 29]. A plastic deformation (or bowing fracture) occurs when a traumatic force produces microscopic failure on the tensile (convex) side of a long bone which does not propagate to the concave side. Consequently the shaft is angulated beyond its elastic limit, resulting in a persistent deformation (Fig. 5.11). The cortex, under the periosteum, has a lower mineral content than the adult one and an increased porosity, due to larger and more abundant Haversian canals; this allows the bone to bent, buckle, or bow but not to break when compressed [13, 15]. In this particular type of injury, there is not an evident fracture line but numerous microfractures on the concave surface of the diaphysis with an intact cortex on the convex side. It is most common in the forearm, especially in the ulna, associated with fracture of the radius, but occasionally it can involve the fibula, the tibia, and the clavicle. Plastic deformation can occur isolated but more commonly it happens together with a fracture of the adjacent bone, meaning that the presence of a fracture in a pediatric skeletal segment should suggest the radiologist to look for deformation in the other one. Sometimes there is a detachment of the periosteal surface with a hematoma. The diagnosis of a bending fracture, often difficult, may be easier using the comparative plain film views [30]. A plastic deformation of the clavicle, consequent to a fall on an outstretched hand or a direct blow to the shoulder, is especially easy to be missed, even with the comparative views, which will show a mild asymmetry of the shafts. A bowing fracture sometimes must be straightened or broken to effect reduction [17, 20, 22]. Buckle fracture (or torus fracture) is the result of a compression failure of bone that usually occurs at the junction of the metaphysis and the diaphysis, where the cortical is less thick, owing to the prevalence of the spongious bone (Fig. 5.12). The term “torus” comes from the Latin word which means swelling which refers to the enlargement that separates the capitellum from the body of the classical column and it is due to the characteristic angulation of the cortex following a pure axial force applied on a hyperextended or hyperflexed bone segment. It is the most common fracture in children and it is easily missed [1, 3], because the only radiological sign is an angled buckle caused by the trabecular compression, while the periosteal and cortical layers on the other side are intact (Fig. 5.13). A typical traumatic mechanism is a fall over an overextended limb with bending of the bone and compression on the concave side: this occurs most commonly at the distal radius following a fall on an outstretched arm. Other common sites for torus fractures are the wrist (Fig. 5.14), the elbow, and the ankle [30]. Buckle (torus) fractures are common in infants and children and generally occur through the metaphyses of long bones (Fig. 5.15). There are two different types of buckle fractures [31]: the classic form and the angled form (Fig. 5.16). The classic form results from axial loading of the long bone with resultant compression of the bone and buckling of the trabeculae along the fracture line. This leads to outward, decompressive, unilateral, or bilateral bulging of the cortex at either end of the fracture line. In the angled form, however, only angulation of the cortex is seen and it usually results from initial axial loading on a long bone but, in addition, associated forces in varus, valgus, hyperextension, or hyperflexion. Depending on which of these is present, the fracture will be seen on the dorsal, ventral, medial, or lateral aspect of the involved long bone [28, 30, 31]. Even if an underlying trabecular compressive fracture is always present in these patients, they usually are not appreciable at the initial time of injury. However, substantiating sclerosis along the fracture zone attests to their presence. Angled buckle fractures usually are isolated, subtle, and easily overlooked. However, once one becomes familiar with their appearance and where they tend to occur, one can diagnose them with more certainty, especially if comparative views are utilized. Soft tissue changes (soft tissue swelling and fat pad obliteration or displacement) also are important as they serve to focus one’s attention on the site of injury and so cause one to look more closely for a possible fracture. Buckle fractures are inherently stable and usually heal in 3–4 weeks with simple immobilization [17, 20, 23]. Greenstick fracture is an incomplete fracture of the metaphysis or diaphysis of the long bones (Fig. 5.17). The name “greenstick” comes from the fracture’s similarity with green, fresh wood which also breaks on the convex side when bent, without a complete line. It occurs when the traumatic force (an angulated longitudinal force or perpendicular force, like a direct blow) causes a disruption of the convex surface of the shaft, but it is not enough to break it completely into separate pieces [3]. It is sometimes associated with plastic deformation on the opposite side. The typical site is the diaphysis or the metaphysis of the wrist. This fracture usually requires immobilization, but if the shaft undergoes a plastic deformation, it is necessary to break the skeletal segment on the concave side to restore a normal alignment, as the plastic deformation recoils the bone back to the deformed position. While the physes are the primary ossification centers (located at the ends of the long bones) and are responsible for longitudinal bone growth, the apophyses are the secondary centers of ossification (found where major tendons attach to bone) and provide contour and shape to growing bones without adding length. Since cartilage is less resistant to tensile forces than bones, ligaments, and muscle-tendon units, these growth centers are the weakest links in the musculoskeletal chain. The same injury mechanisms that cause muscle strains and tendonitis in adults result in growth center injuries in children and teens [32, 33]. Apophyseal injuries usually occur in adolescents playing sports and are often described on the hip bones (ischial tuberosity, iliac spine, pubic ramus, iliac crest, greater and lesser trochanter), the knee (inferior pole of the patella and anterior tibial tubercle), and the spine (secondary ossifying site of the vertebral soma) owing to the greater number of growing plates of these bone districts [34, 35]. Usually they can be diagnosed by history and physical examination and radiographs are needed to rule out fractures or bone lesions, when the presentation is less clear. Utrasonography (US) and magnetic resonance imaging (MRI) play a major role in the definition of the type of lesion and in the depiction of the ligamentous and tendinous compartment [36] (Fig. 5.18). Physeal fractures are those involving the growth plate that is the weakest area in children’s bone and they represent approximately 15 % of all fractures in children. The distal radial physis is the most frequently injured one. Most physeal injuries heal within 3 weeks, and, as a consequence, there is a limited window of time for reduction of deformity. The damage to growth plate may result in progressive angular deformity, limb-length discrepancy, or joint incongruity [18]. The Salter-Harris (S-H) classification continues to be the most commonly used system for characterizing them and it consists of five types of injuries, which are listed by their location (Fig. 5.19). This classification system is important to plan a correct treatment and so to decrease the risk of growth disturbances and angular deformities [33, 37], as children’s bones heal faster than adult ones due to their stronger periosteum. The S-H system divides the fractures into five categories [9, 24] depending upon the type of damage to the growth plate, and a mnemonic way to remember them is the acronym SALTR (slip of physis, type 1; above than physis, type 2; lower than physis, type 3; through the physis, type 4; rammed physis, type 5). Type I S–H fractures (Fig. 5.20) occur when there is a complete separation of the entire physis (usually through areas of hypertrophic and degenerating cartilage cell columns) and the surrounding bone is not involved. Plain X-film appears normal because the physis is radiolucent; reduction and immobilization are needed because healing is rapid and the risk of complications after immobilization is extremely low [33]. Type II S–H fractures are most commonly diagnosed on X-ray (Fig. 5.21); the fracture involves the physis and continues up through a small section of the metaphysis. This fracture is triangle-like and the periosteal layer is torn on the opposite side of the metaphyseal injury, but it is still intact on the adjacent side: the so-called Thurston-Holland sign (Fig. 5.22). After immobilization, healing is usually quick and complications are uncommon [33, 38]. Type III S–H fractures run along the joint surface and persist deep into the epiphyseal plate; they are relatively uncommon and usually they involve the distal tibial or peroneal bone (Fig. 5.23). A surgical approach is often required to ensure proper alignment of the fragments. However, the prospect of recovery is positive as long as the vascular supply to the bone remains intact [19, 33]. Type IV S–H fractures start above the growth plate, in the metaphysis, and cut all the way through the epiphysis (Fig. 5.24); these fractures are usually caused by axial loading or shear stress and comminution is common. Since these fractures damage the joint cartilage, the normal growth of the individual may be impaired and surgery is required in order to properly realign the joint surface [19]. Type V S-H fractures consist in a crushing of the physis; this is the hardest fracture type to diagnose and most difficult to heal. This injury is most likely to occur in the weight-bearing joints of the knee and ankle (Fig. 5.25). Crush injuries result in the disruption of the epiphyseal vascular system and in the death of the growth plate cartilage; this is why type V fractures always have an increased risk of premature fusion [22, 39, 40].


Fig. 5.2
Spiral fracture. Female, 14 years old, after a motor vehicle accident. The anterior X-ray shows a spiral displaced fracture of the diaphyseal tibial shaft (arrow)
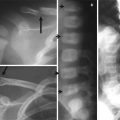
Fig. 5.3




Oblique and transverse fractures. Female, 3 years old, fallen accidentally downward a table. The anterior (a) and the lateral (b) plain films display an oblique fracture of the ulnar shaft (dashed arrow) and a transverse fracture of the radial diaphysis (arrow), both angulated
Related posts:

Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
