This article provides an overview of the imaging evaluation of benign ovarian and adnexal masses in premenopausal and postmenopausal women and lesions discovered during pregnancy. Current imaging techniques are discussed, including pitfalls and differential diagnosis when necessary, as well as management. It also reviews the now well-established American College of Radiology (ACR)/Society of Radiologists in Ultrasound consensus guidelines and covers the more recently introduced Ovarian-Adnexal Reporting and Data System by the ACR and the recently published ADNEx Scoring System.
Key points
- •
Most adnexal masses are benign.
- •
The primary imaging modality for evaluating ovarian and adnexal masses is ultrasonography.
- •
Determining the ovarian or extraovarian origin of a lesion is essential for accurate differential diagnosis and proper management.
- •
When an adnexal mass is indeterminate on ultrasonography, contrast magnetic resonance (MR) imaging is the problem-solving imaging modality of choice.
- •
Adding diffusion-weighted imaging to conventional MR studies may help characterize certain benign ovarian and adnexal lesions.
Video content accompanies this article at http://www.radiologic.theclinics.com .
Introduction
Adnexal disease involves the ovaries, fallopian tubes, and surrounding structures, and is common. Adnexal lesions may be found in symptomatic patients (eg, pelvic pain or palpable pelvic mass) or may be incidentally discovered when imaging for other unrelated conditions. Most adnexal masses are benign, with a reported incidence of up to 20%. This article reviews a variety of benign ovarian and adnexal conditions in premenopausal and postmenopausal women in addition to lesions discovered during pregnancy. Malignant ovarian disease is beyond the scope of this article and will be covered separately under a different article in this issue. Diagnosis and management of benign adnexal masses can be challenging, and this article addresses those issues, as well as examining the new proposed guidelines recently introduced by the American College of Radiology (ACR) Ovarian-Adnexal Reporting and Data System (O-RADS) Committee and the newly published ADNEx Scoring System.
Imaging modalities
The primary imaging modality for evaluating ovarian and adnexal masses is ultrasonography (US), which allows accurate identification in roughly 90% of cases ( Table 1 ). It has the advantage of being readily available, inexpensive, easy to perform (particularly when in the hands of experienced operators), and lacks ionizing radiation. The Women’s Imaging ACR Appropriateness Criteria Committee rates US with duplex Doppler as usually appropriate when initially assessing for a gynecologic or nongynecologic cause in women presenting with acute pelvic pain or when an adnexal mass is clinically suspected. No other imaging modality had shown better diagnostic capabilities than US as a first-line diagnostic imaging tool when an adnexal mass was suspected.
| Imaging Modalities | Advantages | Disadvantages |
|---|---|---|
| US | Easy to perform Widely available Low cost No ionizing radiation Excellent screening tool | Operator dependent Some degree of expertise needed for interpretation Some masses may remain indeterminate |
| MR imaging | Problem-solving tool for indeterminate US findings Excellent soft tissue resolution Can be used in pregnant patients | Not readily available Costly Limited by patient size and claustrophobia |
| CT | Used for malignancy staging | Ionizing radiation Poor soft tissue discrimination of adnexae |
| PET/CT | No role in evaluation of benign adnexal disease | Ionizing radiation |
Combining a transabdominal and transvaginal (TV) approach allows identification of large pelvic masses extending into the lower abdomen as well as deep-seated pelvic masses in the cul-de-sac. TV US has a reported sensitivity and specificity of 93.5% and 91.5% respectively in differentiating benign from malignant adnexal masses. Although three-dimensional (3D) US is being used increasingly in the diagnostic work-up of female pelvic disease, two-dimensional (2D) US remains the principal technique used in daily practice. Color Doppler is a paramount adjunct to gray-scale imaging. However, its sensitivity in distinguishing between benign and malignant lesions remains low, varying between 50% and 80%, with a slightly higher specificity ranging between 80% and 90%. Real-time contrast-enhanced US can improve characterization of otherwise indeterminate ovarian lesions found on conventional 2D gray-scale US by observing both the degree and timing of enhancement of solid components. Zhang and colleagues found that transabdominal contrast-enhanced US evaluation of malignant ovarian masses showed both faster and more enhancement than benign lesions. They also observed that the pattern of enhancement was more inhomogeneous in 44 out of 48 of their malignant ovarian lesions compared with only 5 out of 72 benign masses. In their study of 51 ovarian lesions, Szymanski and colleagues showed similar results using contrast-enhanced TV US, confirming that the presence of neovascularity in lesions could predict malignancy. Hu and colleagues combined TV 2D and 3D contrast-enhanced US to differentiate small benign from malignant adnexal masses and achieved a diagnostic sensitivity of 100%.
Computed tomography (CT) is not the preferred imaging modality in the initial evaluation of the female pelvis and it is not ideal for imaging pregnant patients or for follow-up of any known adnexal disorder other than in cases of staging and preoperative planning for ovarian cancer. The Women’s Imaging ACR AC Committee rates the use of CT with or without intravenous contrast as usually not appropriate in the initial evaluation of a suspected gynecologic adnexal mass or follow-up of a known adnexal mass. , This is principally because its soft tissue discrimination of the adnexal region is extremely poor and it also exposes the female pelvis to potentially harmful ionizing radiation. However, the increasing use of multidetector CT imaging in everyday clinical practice has led to incidental discovery of many adnexal lesions in patients being imaged for other reasons. It is therefore important to recognize CT findings that are particular to certain adnexal disorders and, more importantly, to recommend the appropriate next imaging modality because this is common practice. “Management of Incidental Adnexal Findings on CT and MRI: A White Paper of the American College of Radiology Incidental Findings Committee” revised guidelines are in press at the time of completion of this article.
Contrast-enhanced CT has been found to have a diagnostic accuracy comparable with US and magnetic resonance (MR) imaging in differentiating malignant from benign lesions.
MR imaging is an excellent cross-sectional imaging tool to better characterize adnexal masses that are indeterminate on US either based on atypical sonographic features or the inconclusive organ of origin. It is also ideal for imaging pregnant patients given its lack of ionizing radiation to the fetus. Approximately 5% to 25% of adnexal masses are still classified as indeterminate following US evaluation. MR imaging is particularly helpful because of its superior soft tissue contrast and resolution and its multiplanar imaging capabilities, with reported overall accuracy of up to 95% in differentiating benign from malignant ovarian masses. The acquisition of different series, such as T1-weighted and T2-weighted sequences, chemical shift sequences, and fat-suppressed sequences, allows identification of specific tissue types, such as fluid, hemorrhage, fat, or solid/fibrotic components. The adjunct of intravenous (IV) contrast with dynamic imaging allows the evaluation of vascularity and enhancement of septations, internal mural nodules, or papillary projections. MR imaging with IV contrast has been found to be the next best imaging study when an incidentally found ovarian mass remains indeterminate on US, being a highly specific test given its ability to diagnose benign disease. Functional MR imaging techniques such as diffusion-weighted and perfusion-weighted sequences have been reported to be valuable in distinguishing benign from malignant ovarian lesions. , In 2016, the European Society of Urogenital Radiology (ESUR) published new recommendations for MR imaging characterization of indeterminate ovarian masses on US. They recommended combining the use of diffusion-weighted imaging (DWI) with a high b value with T2-weighted sequences to diagnose certain solid benign ovarian and adnexal lesions. They found that lesions that were hypointense on T2 and DWI regardless of their enhancement pattern had a high likelihood of being benign, an observation that is particularly helpful during pregnancy given that MR contrast is contraindicated.
There is no documented role in the literature for the use of PET/CT imaging in the initial evaluation or follow-up of a known or suspected benign adnexal mass in premenopausal or postmenopausal and pregnant women.
Imaging diagnosis of benign ovarian and adnexal lesions
Across imaging modalities, adnexal masses can be classified as cystic, solid, or mixed solid/cystic. In 2010 and 2019, the Society of Radiologists in Ultrasound (SRU) published diagnostic guidelines and follow-up recommendations for asymptomatic ovarian and adnexal cystic lesions in premenopausal and postmenopausal women, excluding solid masses. , Table 2 summarizes their recommendations.
| Ovarian Lesion | Premenopausal | Postmenopausal |
|---|---|---|
| Follow-up | ||
| Simple cyst | >5 cm and ≤7 cm: none | >3 cm and ≤5 cm: none |
| >7 cm: additional imaging at 2–6 mo for further characterization or 6–12 mo for growth assessment | >5 cm: additional imaging at 3–6 mo for further characterization or 6–12 mo for growth assessment | |
| Hemorrhagic cyst | ≤5 cm: none | Early menopause: any size should be followed up to confirm resolution |
| >5 cm: 6–12 wk to confirm resolution | Late menopause: consider surgical evaluation | |
| Endometrioma | First follow-up at 6–12 wk then yearly unless removed surgically | First follow-up at 6–12 wk then yearly unless removed surgically |
| Dermoid cyst | Follow-up yearly unless surgically removed | Follow-up yearly unless surgically removed |
Benign ovarian lesions
Simple Ovarian Cysts
Most simple cysts are benign functional cysts. When an US diagnosis of simple cyst is made, a benign process is established in 98.7% and 100% of premenopausal and postmenopausal women respectively. , Furthermore, Valentin and colleagues evaluated the risk of malignancy of 1148 unilocular cysts at TV imaging and found it to be 0.96% overall in premenopausal and postmenopausal women.
Most simple cysts in premenopausal women are either follicular or corpus luteum cysts measuring less than or equal to 3 cm and resolve without intervention. During the menstrual cycle, follicular cysts enlarge progressively through the proliferative phase with 1 dominant follicle becoming mature and largest by ovulation time. If ovulation fails, the follicle continues to enlarge, becoming a functional cyst that can reach up to 20 cm. Simple cysts have an imperceptible smooth wall, with no internal septations, mural nodularity, or papillary projections. They are anechoic on US, showing posterior acoustic enhancement, and are avascular on color Doppler. On CT and MR imaging, cysts have simple fluid attenuation density and intensity respectively. Corpus luteum cysts are seen after ovulation and represent the residua of an involuting follicle ( Fig. 1 ).

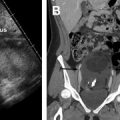
Other simple cystic ovarian lesions include serous cystadenomas, theca lutein cysts, and polycystic ovaries. Serous cystadenomas are subtypes of epithelial ovarian tumors and represent up to 25% of all benign ovarian neoplasms. They are often seen in women 40 to 50 years of age and are one of the most common simple cystic ovarian lesions found in postmenopausal women at surgery. They present on imaging as unilateral or bilateral unilocular cysts, may be as large as 50 cm, and persist on follow-up imaging ( Fig. 2 ). Theca lutein cysts consist of multiple unilocular cysts and are the result of increased levels of beta-human chorionic gonadotropin (β-hCG) in the setting of gestational trophoblastic disease, multiple pregnancies, or ovarian hyperstimulation during assisted reproduction therapy. US shows bilateral ovarian enlargement caused by the presence of numerous unilocular follicles of varying size ( Fig. 3 ). On CT and MR imaging, the ovaries may have a spoke-wheel appearance with the follicles arranged peripherally surrounding the more central ovarian stroma. The cysts regress spontaneously later in the pregnancy or after delivery. In the setting of hyperreactio luteinalis, which is a result of hypersensitivity to circulating hCG levels in the absence of ovulation induction treatment, the ovaries have a similar appearance. The diagnosis is usually suggested by the timing, occurring in the third trimester, as well as by the presence of maternal virilization, seen in up to 25% of cases. Polycystic ovaries also contain multiple cysts; however, their appearance differs from theca lutein cysts based on the number and size of the individual cysts. Ovarian volumes do not necessarily help in differentiating between the 2 entities because polycystic ovaries may or may not be enlarged. According to the American College of Obstetricians and Gynecologists (ACOG) guidelines, the imaging diagnosis of polycystic ovaries is made if 1 or both ovaries contain 12 or more small follicles measuring 2 to 9 mm and if the ovarian volume is greater than 10 cm 3 . Although roughly 23% of premenopausal women have polycystic-appearing ovaries, only about 5% to 10% have symptoms of polycystic ovarian syndrome (PCOS), which is an endocrinologic disorder with chronic anovulation caused by an imbalance in follicle-stimulating and luteinizing hormones. Patients with PCOS often present with infertility, amenorrhea, obesity, and hirsutism. The US and MR imaging appearance of polycystic ovaries is characteristic, with numerous peripherally arranged small follicles in a classic string-of-pearls pattern ( Fig. 4 ).



Not Simple Ovarian Cysts
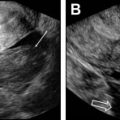
Endometriomas are characterized by the presence of active ectopic endometrial tissue outside the uterus and may have a range of appearances on imaging. They have been referred to as chocolate cysts because of their dark, thick, gelatinous content, which represents aged blood products. The classic US findings are those of a unilocular thick-walled homogeneous cyst containing multiple low-level ground-glass echoes ( Fig. 5 ). This appearance was described in 95% of endometriomas by Patel and colleagues in a retrospective review of 252 adnexal masses. Additional sonographic findings described in typical endometriomas include hyperechoic foci in the cyst wall or multilocularity. Endometriomas may have a more atypical appearance in pregnancy and postmenopausal women. These appearances include multiple septations, fluid-fluid levels, and central calcifications ( Fig. 6 A). , Decidualized endometriomas seen during pregnancy may develop solid vascular mural nodules mimicking neoplasms ( Fig. 6 B). , Some helpful distinguishing imaging features that have been suggested for making a prospective diagnosis include vascular solid nodules with smooth lobulated margins noted early in pregnancy and without showing significant change in size, and a similar appearance to the decidualized endometrium. , It is important to recognize these less common atypical features in order not to overdiagnose or overlook malignant transformations of endometriomas into endometrioid carcinomas or clear cell carcinomas, which can occur in up to 1%. Malignant transformations should be suspected if a known endometrioma shows rapid enlargement and interval development of solid vascular components. On MR imaging, endometriomas have homogeneous high signal intensity on T1-weighted fat-suppressed sequences and low signal on T2-weighted sequences, referred to as T2 shading (see Fig. 5 ). They may have a T2 dark fibrous wall that enhances after contrast administration without any mural nodularity or enhancement of central contents. When such a lesion shows these MR characteristics, a diagnosis of endometrioma can be made with a higher than 90% specificity. Malignant transformation is better diagnosed on dynamic subtraction images ( Fig. 7 ). Compared with hemorrhagic cysts’ signal intensity on MR imaging, endometriomas tend to have higher T1 and lower T2 signal characteristics, which is thought to be caused by their higher protein concentration and increased viscosity. In addition, Corwin and colleagues showed that findings of a T2 dark spot on MR imaging within cystic adnexal masses helped establish a diagnosis of endometrioma with a specificity of 93% and a positive predictive value of 98%. However, distinguishing between the 2 entities on conventional MR imaging can be challenging at times given the overlapping imaging characteristics of blood products, and it has been suggested that using apparent diffusion coefficient (ADC) values would be helpful in making that distinction. In their study of 25 women, Balaban and colleagues observed that endometriomas had significantly lower ADC values compared with hemorrhagic cysts, with a higher sensitivity and specificity at b 1000.



Hemorrhagic cysts are thought to be the result of bleeding into corpus luteum cysts. Patients usually present with acute pelvic pain and US allows a definitive diagnosis in most cases ( Fig. 8 ). Most hemorrhagic cysts resolve over time and do not need additional confirmatory imaging. However, when incidentally discovered on MR imaging, they may have similar signal characteristics to endometriomas with a few discriminating features: hemorrhagic cysts are often more heterogeneous than endometriomas and they are less T1 hyperintense and less T2 hypointense. When they rupture, they can result in hemoperitoneum of variable amount in the pelvis and upper abdomen ( Fig. 9 ). It is important to exclude the possibility of a ruptured ectopic pregnancy in this setting given that patients may present with similar symptoms and imaging findings. Hemorrhagic cysts are not encountered in late menopausal women because they no longer ovulate and, if similar-appearing cysts are found at imaging, these patients need surgical evaluation to exclude a neoplastic lesion. However, these cysts can still occur in perimenopausal and early postmenopausal women; in this patient population a 6-week to 12-week interval follow-up with US is recommended to ensure resolution.


Related posts:
 Imaging Safety and Technical Considerations in the Reproductive Age Female
Imaging Safety and Technical Considerations in the Reproductive Age Female
 Magnetic Resonance Imaging of the Female Pelvic Floor
Magnetic Resonance Imaging of the Female Pelvic Floor
 Imaging of Acute Pelvic Pain
Imaging of Acute Pelvic Pain
 Integrated MR Analytical Approach and Reporting of Pelvic Floor Dysfunction
Integrated MR Analytical Approach and Reporting of Pelvic Floor Dysfunction
 Imaging of Postpartum/Peripartum Complications
Imaging of Postpartum/Peripartum Complications
 Nonfetal Imaging During Pregnancy
Nonfetal Imaging During Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


