Abstract
The craniovertebral junction is formed by the occipital bone, atlas, and axis. It is a complex structure and consists of osseous, soft tissue, and nervous system. In this chapter, we focus on illustrating the lesions involving the craniovertebral junction. They include congenital anomalies, fractures of special type, degenerative disorders, infectious/inflammatory diseases, tumor and its mimics, and also common vascular lesions occurring in this particular anatomic region. Rare and clinically irrelevant lesions are excluded.
Keywords
Congenital, Craniovertebral junction, Degeneration, Fracture, Infection, Tumor, Vascular
The craniovertebral junction (CVJ) supports the head and enables its flexion and rotation in three dimensions. It has a complex anatomic structure consisting of the vertebral column, paraspinal soft tissue, ligaments, and joints between the clivus, occipital bone, foramen magnum, atlas (C1), and axis (C2). In this chapter, we emphasize and discuss mainly on CVJ disorders with clinical significance.
Embryology and Congenital Anomalies
Embryonic development of the CVJ has been discussed in detail in many previous reports. In brief, a total of 42 somites are formed in the fourth week of gestation. Each somite differentiates into three parts (the outer dermatome, inner myotome, and medial sclerotome). The medial sclerotomes form the vertebral bodies. Generally, the upper half of one sclerotome unites with the lower half of its neighbor to form the vertebral body. Yet, the first four sclerotomes (first occipital, second occipital, third occipital, and fourth proatlas) follow a different course, ending in the formation of the basiocciput, exoccipital centers (i.e., the lateral margins of the foramen magnum, occipital condyles, and hypoglossal canal), jugular tubercles, posterior portions of the foramen magnum, most of the C1, and apex of the C2 dens. The first spinal sclerotome forms the C1 posterior arch and body of the C2 dens, whereas the second spinal sclerotome forms the body, facets, and posterior arch of the C2. Patients are prone to develop multiple congenital anomalies of the CVJ owing to the complexity of embryonic development.
Measurement Commonly Used in Evaluating the Craniovertebral Junction
In the era of plain X-ray examination, many measurements have been proposed for evaluating the alignment of the CVJ ( Table 14.1 ; Fig. 14.1 ). In this chapter, however, we emphasize the application of computed images including computed tomography (CT), magnetic resonance imaging (MRI), and digital subtraction angiography (DSA), they still can be applied.
| Fig. 14.1 | Normal Range | Remarks | |
|---|---|---|---|
| Chamberlain line (Palatooccipital line) | A to B | Dens apex < 5 mm above this line, anterior arch of C1 typically lies below | Diagnosis of basilar invagination. (Posterior rim of foramen magnum shows great anatomic variability and also it may be difficult to radiologically pinpoint opisthion) |
| McGregor line (Palatosuboccipital line) | A to C | Dens apex < 7 mm above this line, anterior arch of C1 typically lies below | Diagnosis of basilar invagination |
| McRae line (Foramen magnum line) | B to D | Tip of dens below this line | Assess the decrease in content injury |
| Wackenheim line (craniovertebral or clivus-canal angle) | D to E | Line falls tangent to, or intersects, the posterior one-third of the odontoid | Assessment of CVJ traumatic injuries |
| Welcher basal angle | Angle D-F-G | <140 degrees | Assessment of platybasia |

Congenital Anomalies
Depending on the location of the involved sclerotomes, congenital anomalies can be divided into three groups (see Box 14.1 ). In the same individual, single or multiple anomalies can exist and can involve osseous, neural, and vascular components. Anomalies including malsegmentation, failure of fusion of different components of each bone, hypoplasia or agenesis, and ankyloses arise from insults occurring between the fourth and seventh week of intrauterine life.
Malformations of the occipital bone
- 1.
Platybasia
- 2.
Basilar invagination (basioccipital hypoplasia)
- 3.
Condylar hypoplasia
- 4.
Condylar dysplasia (condylus tertius, paracondyloid process, and basilar process)
Malformations of the atlas
- 1.
Atlas assimilation
- 2.
Aplasia and hypoplasia of the atlas
- 3.
Atlas arch anomaly
- 4.
Ponticulus posticus
Malformations of the axis and odontoid process
- 1.
Aplasia or hypoplasia of the dens
- 2.
Persistent ossiculum terminale
- 3.
Os odontoideum
- 4.
Klippel-Feil anomaly
Malformations of the Occipital Bone
Platybasia
Platybasia is an anthropometric term referring to the flattening of the skull base resulting in an increase in the Welcher basal angle (>143–145 degrees). Platybasia alone does not usually cause symptoms unless it is associated with basilar invagination or other anomalies.
Basilar Invagination (Basioccipital Hypoplasia, Basilar Impression)
Basilar invagination implies that the floor of the skull is pressed in by the dens and the tip of the odontoid is more cephalad and protrudes into the foramen magnum, resulting in compression of the brainstem or its neurovascular structures. Most patients with basilar invagination actually have a normal basal angle and thus do not have associated platybasia. Basilar invagination is divided by etiology into two types: primary or developmental invagination, which is more common, and secondary or acquired invagination.
Developmental invagination is associated with atlantooccipital assimilation, hypoplasia of the basiooccipital or atlas, incomplete fusion of the posterior arch of the atlas, odontoid anomalies, Klippel-Feil syndrome, and vertebral artery anomalies. In about 25%–35% of cases, basilar invagination is associated with Arnold-Chiari malformation, syringomyelia, and hydrocephalus. The symptoms and signs of developmental basilar invagination usually occur in the second or third decade. The most common local finding is short neck and torticollis. The patients might have symptoms and signs of increased intracranial pressure because of blockage of cerebrospinal fluid (CSF) circulation or vertical or lateral nystagmus because of compression of the cerebellum and vestibular apparatus. Some patients present with vertebral artery insufficiency.
Our and previous observations indicate there may be two different types of developmental basilar invaginations based on imaging findings. One group of patients had classical imaging findings ( Fig. 14.2 ) of odontoid process protrusion into the foramen magnum in the cephalad direction, C1-2 dislocation or dens-clivus dislocation causing direct compression of the pontomedullary junction with violation of the Chamberlain, McRae, and Wackenheim lines, and listhesis of the oblique C1 and C2 facets. The other group of patients had imaging findings such as horizontal orientation of the clivus and anatomic alignment of the odontoid process and clivus despite the presence of basilar invagination, violation of the Chamberlain line but not the McRae and Wackenheim lines, and normal or fused horizontal C1-2 facet joints. This type of developmental basilar invagination is considered to be related to atlantoaxial dislocation stemming from aplasia and hypoplasia of the atlas. For details, please see the following section.
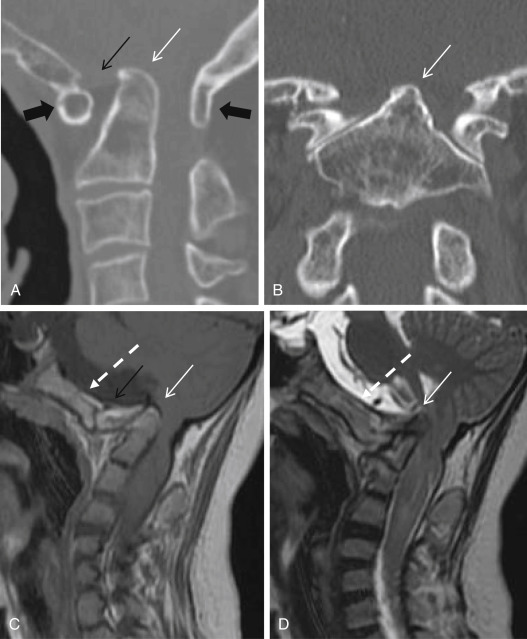
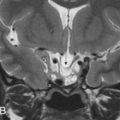
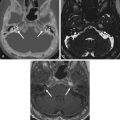
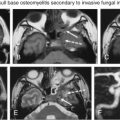
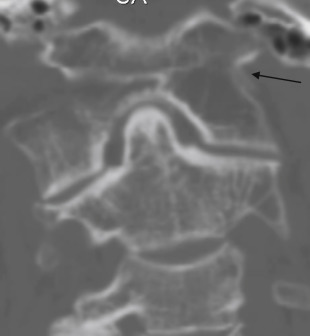
Acquired basilar invagination may be due to general osteopenia (Paget disease, osteomalacia, renal osteodystrophy, and hyperparathyroidism), local bone destruction (from a primary or secondary tumor or infection) ( Fig. 14.3 ), trauma, and systematic diseases such as osteogenesis imperfecta, achondrodysplasia, osteopetrosis, mucopolysaccharidosis, and cretinism.

Condylar Hypoplasia
In condylar hypoplasia, the occipital condyles are underdeveloped and have a flattened appearance; as a result, the skull base is flattened or even ascends medially, leading to basilar invagination and widening of the atlantooccipital joint axis angle. The lateral masses of the atlas may be fused to the hypoplastic condyles and further accentuate the basilar invagination.
Condylar hypoplasia restricts movement at the atlantooccipital joint and may lead to compression of the vertebral artery because of posterior sliding of the occiput in relation to the atlas.
Condylar Dysplasia (Condylus Tertius, Third Occipital Condyle)
Condylar dysplasia is characterized by persistence of the proatlas (the hypochordal bow of the fourth occipital sclerotome) or its failed integration into the occipital bone. This leads to an ossified remnant present at the distal end of the clivus.
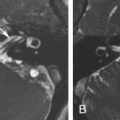
It is usually directly above and anterior to the arch of C1 and may form a joint or pseudojoint with the clivus, odontoid process, or anterior arch of C1 ( Fig. 14.4 ). Occasionally, it can cause limitation in the range of motion of the CVJ.

Malformations of the Atlas
Atlas Assimilation (Atlantooccipital Assimilation, Occipitalization of the Atlas)
Atlas assimilation refers to complete or partial congenital fusion of C1 with the occiput. It results from failure of segmentation between the fourth occipital sclerotome and first spinal sclerotome. The most common form of atlas abnormality is atlas assimilation, which is fusion of the anterior arch of C1 with the lowest end of the clivus ( Fig. 14.2A and B ). It may be unilateral ( Fig. 14.5 ), segmental, focal, or bilateral. Bilateral atlas assimilation invariably leads to basilar invagination. It occurs commonly in conjunction with other abnormalities such as Klippel-Feil syndrome. When this is present, especially in the second and third cervical vertebrae ( Fig. 14.6 ), there is a gradual loosening of the atlantoaxial joint, and the atlantoaxial subsequently becomes unstable. Sudden death has been reported in a patient with atlas assimilation.

Aplasia and Hypoplasia of the Atlas
Most isolated atlas anomalies are benign except the atlantal assimilations mentioned earlier. They produce no abnormal CVJ relationships and are not associated with basilar invagination. CT shows that several ossification centers participate in atlas development. The lateral atlantal masses must be present at birth, and the neural ring must be formed by the age of 3 years. Abnormal atlantal development is observed in skeletal dysplasia syndromes (spondyloepiphyseal dysplasia, achondroplasia, Goldenhar syndrome) and in genetic abnormalities (Down syndrome).
A persistent bifid anterior and posterior arch of the atlas beyond the age of 3–4 years is observed in skeletal dysplasias, mucopolysaccharidosis, Down syndrome, Goldenhar syndrome, Conradi syndrome, Morquio syndrome, and atlas assimilation. The presentation is torticollis and plagiocephaly. Without proper management, this subsequently results in atlantoaxial subluxation (AAS). Down syndrome is associated with a 14%–20% incidence of atlantoaxial dislocation. This developmental and slow-in-coming acquired change may subsequently evolve into basilar invagination.
In the initial stage, atlantoaxial instability is reducible. The pannus, a prolific granulation tissue mass, surrounds the odontoid process providing protection and preventing the upward motion of the dens into the irreducible basilar invagination until the individual reaches the age of 14–15 years. However, compression of the cervicomedullary junction may cause the clinical symptoms and signs.
In the irreducible basilar invagination ( Fig. 14.7 ), the CVJ emerges from the abnormal groove behind the occipital condyles and pushes up into the cranial base, resulting in platybasia and a short horizontal clivus. The upward excursion of the cranial base and the decrease of the vertical height of the posterior fossa leads to an acquired hindbrain herniation syndrome. The treatment of reducible, irreducible, and acquired hindbrain herniation syndrome are completely different.

Atlas Arch Anomaly
Total or partial aplasia of the posterior atlas arch is rare, but clefts in the atlas arches are much more common, with posterior clefts being the most common and apparent in 4% of adults. The majority of posterior atlas clefts (97%) are midline. Bilateral atlas posterior clefts may resemble the Jefferson fracture. Anterior arch clefts are quite rare (0.1%) and usually associated with posterior clefts (split atlas). In Down syndrome, split atlas occurs frequently and is associated with os odontoideum and the subsequent formation of AAS.
On a lateral radiograph of the upper cervical spine, the predental space sits between the anterior arch of the atlas (which appears to be crescent, or half-moon, shaped) and the dens. In the anterior arch cleft, the predental space is obscured by the anterior arch, which becomes fatty and round and appears to overlap the dens.
Ponticulus posticus (Kimmerle deformity, sagittale foramen, atlantal posterior foramen, arcuate foramen, upper retroarticular foramen, canalis vertebralis, retroarticular vertebral artery ring, retroarticular canal, and retrocondilar vertebral artery) is a bony arch located between the posterior portion of the superior articular process and the posterolateral portion of the superior margin of the posterior arch of the atlas and is formed by ossification of a portion of the oblique atlantooccipital ligament. It may be only a few millimeters long or if longer may produce a foramen through which the V3 portion of the vertebral artery passes. The incidence of ponticulus posticus is about 8% (range 2.6%–14.3%), and it is slightly more common in females. It can be complete, incomplete, or calcified and may be unilateral or bilateral ( Fig. 14.8 ). Complete ponticulus posticus may cause chronic tension-type headache, orofacial pain, and migraine, and its relationship to Bow hunter syndrome (BHS) is unclear.

Malformations of the Axis and Odontoid Process
Aplasia or Hypoplasia of the Dens
Total aplasia of the odontoid process is extremely rare. It can be identified as an extension of the dens to just above the lateral articular masses, with its tip lying below the level of the superior margin of the C1 anterior arch. The attachments for the apical and alar ligaments are absent in aplasia and hypoplasia of the odontoid and predisposing to atlantoaxial dislocation. Odontoid aplasia has been reported to have an association with a variety of congenital dysplastic syndromes such as Morquio syndrome, spondyloepiphyseal dysplasia, and metatrophic dwarfism.
Persistent Ossiculum Terminale (Bergmann Ossicle)
Persistent ossiculum terminale results from nonfusion of the terminal ossification center with the remnant of the odontoid process ( Fig. 14.9 ). It has to be differentiated from type I odontoid fracture (avulsion of the terminal ossicle). The odontoid process is usually of normal height. This anomaly is stable when isolated and of little clinical significance.

Ossiculum Odontoideum (Os Odontoideum)
Os odontoideum is an independent bone lying cranially to the C2 body in place of the dens. Radiographically, the os odontoideum has smooth borders and a small dens is always present. The anterior arch of C1 may appear rounded and hypertrophic. Os odontoideum is located in the same position as the dens near the clivus, with which it may fuse. The gap between the os odontoideum and the C2 usually extends above the level of the superior facets of the C2 ( Fig. 14.10 ).

There are two types of os odontoideum. The first (type A, the orthotopic type) is defined by relocation of the os odontoideum to the site of the dens and movement of the os odontoideum with the C1 and C2 vertebrae. The second (type B, the dystopic type) is defined by relocation of the os odontoideum to a site near the skull base and movement of the os odontoideum with the clivus. The entire complex leads to an incompetence of the cruciate ligament and, subsequently, to atlantoaxial instability. In extreme cases, the os odontoideum may become fixed and associated with severe basilar invagination and compression of the cervicomedullary junction.
Klippel-Feil Anomaly
Klippel-Feil anomaly is a congenital fusion or malsegmentation of the cervical spine. It is due to failure of normal segmentation of the cervical somites between the third and eighth weeks of gestation. Klippel-Feil anomaly can be localized, multisegmental, or diffuse. In the involved segment, the disk space may be absent or hypoplastic, and vertebral bodies become narrow or flat and wide ( Figs. 14.6, 14.10, and 14.11 ). This finding is not obvious in infancy because of incomplete ossification. Klippel-Feil anomaly can occasionally involve posterior elements such as the lamina.

Less than 50% of cases present with the classic triad of short neck, webbed neck, and low hairline. Many associated symptoms and signs have been noted, including deafness, high arch palate, facial palsies, facial asymmetry, torticollis, ptosis of the eye, Duane eye contracture, abnormal rib fusion, scoliosis, syndactyly, hypoplastic thumb, supernumerary digits, hypoplasia of the upper extremity, genitourinary tract abnormalities, and cardiovascular abnormalities.
Fracture
Basilar skull fractures are defined as linear fractures in the skull base, and are usually a part of multitude of facial fractures that extend to the skull base. CVJ fracture can occur in four major elements of its anatomic organization.
Clivus Fracture
Clivus fractures are uncommon, with an incidence of 0.21%–0.56% among patients with head trauma, usually high-energy blunt head trauma. The diagnosis of clivus fracture from plain radiographs is difficult because of the overlaying dense petrous temporal bones. In one study, high-resolution CT scanning with multiplanar reconstruction revealed clivus fracture in 9 (0.36%) of 2500 patients with head trauma. Clivus fracture can be longitudinal, transverse, or oblique and result in cranial nerve deficits (cranial nerves VI and VII) and vascular complications.
Mortality is high (24%–31%) because of brain stem trauma and carotid or vertebrobasilar occlusion. Transverse and diastatic fractures are associated with a higher mortality rate and worse outcome.
Occipital Condyle Fracture
Occipital condylar fractures tend to be high-energy blunt traumas. Because occipital condylar fracture may be asymptomatic or masked by death or concomitant injuries or have delayed manifestations, the true incidence is difficult to determine. One report suggests that the incidence of craniocervical injury might be as high as 16%.
Diagnosis of fracture of the occipital condyle requires a high index of suspicion and high-resolution tomography. Occipital condyle fracture should be suspected when paralysis of the 9th through the 12th nerves (Collet-Sicard syndrome) occurs after minor head trauma. These fractures are divided into three types (see Box 14.2 ).
Type 1 fractures result from axial compression with comminution of the occipital condyle, and the intact alar ligaments and tectorial membrane tend to stabilize the craniovertebral junction (CVJ).
Type 2 fractures result from a direct blow to the skull base and occipital condyle, and the intact alar ligaments tend to stabilize the CVJ.
Type 3 fractures result from avulsion, and the torn alar ligaments tend to destabilize the CVJ.
It has been well established that conventional radiographs alone miss up to half of patients with acute craniocervical instability. Patients with occipital condyle fractures may have a wide variety of clinical outcomes and high incidence of additional cervical spine injuries affecting neurologic outcome.
Atlas Fracture
Atlas fractures account for 2%–13% of acute injuries of the cervical spine (see Box 14.3 ), are due to a traumatic axial load, and are typically associated with other damage to the upper cervical spine. C1 anterior ring fractures are not an uncommon finding, and a prevertebral soft tissue thickness of >10 mm on radiography is highly suggestive of such a fracture. Definitive diagnosis of an isolated fracture often requires CT scans ( Fig. 14.11 ), whereas ligamentous injury is most readily identified with MRI. The distance between the atlas and the dens (atlantodens interval, ADI) is a marker for ligamentous instability. Normally, ADI is <3 mm in adults (<5 mm in children), but when it is 3–5 mm in adults, injury to the transverse ligament with intact alar and apical ligaments is suggested. ADI >5 mm in adults indicates serious injury to the transverse ligament, alar ligament, and tectorial membrane (atlantoaxial subluxation or dislocation). In children, the C1 body may not be visualized radiographically until patients reach 1 year of age and does not fuse until they reach 4 years of age.
Type I—fractures that are limited to the anterior or posterior arch, with intact transverse ligament
Type II—fractures (also known as Jefferson fractures) that typically consist of bilateral burst fractures through the anterior and posterior arches of C1
Type III—fractures that involve the lateral mass
Jefferson fractures (type II) ( Fig. 14.12 ) and lateral mass fractures (type III) may occur in isolation or in conjunction with significant ligamentous disruption. If the sum of lateral mass displacement is >7 mm, then a transverse ligament rupture is assured and the injury pattern is considered unstable. MRI is more sensitive at detecting injury to transverse ligaments. Vertebral artery injuries are assessable with neck computed tomography angiography (CTA) when atlas fracture is diagnosed. If a vertebral artery dissection is found, the patient will need anticoagulation with heparin and further evaluation by interventional radiology.

Axis Fracture (Odontoid Fracture)
The incidence of odontoid fractures approaches 15% of all C-spine fractures (see Box 14.4 ). Usually, these fractures are secondary to motor vehicle accidents or falls. When an odontoid fracture is suspected, it is important to rule out concomitant associated C-spine injuries.
Type I—an oblique fracture through the upper part of the odontoid process
Type II—a fracture occurring at the base of the odontoid as it attaches to the body of C2
Type III—a fracture that extends through the body of the axis
A type I fracture (less than 5% of cases) usually is stable if limited to an avulsion injury to the tip of the odontoid process. Occasionally, the apical and/or alar ligaments are injured as a result of traction forces and become unstable. More than 60% of odontoid fractures are type II fractures ( Fig. 14.13 ). A type III fracture (30% of cases) can extend laterally to the superior articular facet of the atlas and develop vertically in the odontoid process and body of the axis (less than 5% of cases). An isolated C2 lateral mass fracture is extremely rare, and if found, other C-spine pathology must be sought.

Hangman fracture ( Fig. 14.14 and Box 14.5 ) involves the pars interarticularis and adjacent structures and results from hyperextension injury.

Type 1—an isolated minimally displaced fracture of the ring without displacement of the body or facets
Type 2—a fracture of the pars with anterior displacement of the axial body
Type 3—a fracture of the pars with anterior displacement of the axial body in the direction of flexion and dislocation of the bilateral facets
Degenerative Lesions of the CVJ
The degenerative lesions in the CVJ include degenerative arthritis (osteoarthritis), ossification of the posterior longitudinal ligament, and diffuse idiopathic skeletal hyperostosis (DISH). The retroodontoid pseudotumor (ROP) (which might be associated with various kinds of degenerative or inflammatory arthritis in the CVJ region) is discussed herein.
Degenerative Arthritis
Degenerative arthritis of the CVJ is not uncommon but is easily neglected because the lower cervical spine degeneration is more prevalent and causes more specific symptoms such as radiculopathy. Atlantoaxial osteoarthritis is an underrecognized source of neck pain, limitation of range of motion, and cervicogenic headaches. The complex anatomy of the occiput-atlas-axis complex and the wide range of motion at the occipitocervical junction and atlantoaxial joints render them susceptible to multiple degenerative and traumatic processes. The incidence of degenerative arthritis of the CVJ increases with age. An earlier study using radiographs reported that the prevalence of severe lateral atlantoaxial osteoarthritis ranges from 5.4% in the sixth to 18.2% in the ninth decade of life. A more recent prevalence study using CT in a group of 1543 adult subjects (aged 18–103 years) found osteoarthritis of the anterior atlantodens joint in 44.6% and that with age, a significant increase occurs in the prevalence of degenerative changes at the atlantoaxial joint, ranging from 1.4% in the youngest group to 92.9% in the oldest group. They found that, with age, the ADI narrowed linearly, the prevalence of intraosseous cysts increased exponentially from 4.2% to 37.4%, and the prevalence of calcific synovitis increased from 0% to 11.1%. Degenerative arthritis could be primary or secondary to trauma or even osteoradionecrosis (ORN) related to prior irradiation for head and neck cancer. The degenerative arthritis at the CVJ may involve the lateral atlantoaxial joint (usually unilateral or bilateral asymmetric), the midline atlantoodontoid joint, and the occipitocervical joint. C1-C2 facet osteoarthritis is symptomatic in 4% of patients with known peripheral or spinal osteoarthritis, occurring in females at 74%, and presenting unilaterally in 76% in one large series. Degenerative arthritis of the CVJ might also cause craniovertebral instability and resultant myelopathy. Surgical decompression and atlantoaxial fusion might be considered for managing refractory cases.
The imaging findings are similar to those seen in degenerative arthritis elsewhere in the body, including marginal osteophyte formation, joint space narrowing, subchondral sclerosis, and subchondral cyst formation ( Fig. 14.15 ). These findings are commonly associated with varying degrees of lateral mass collapse, ligamentous thickening, or calcification. Further radiologic features associated with craniovertebral instability include reduction in the height of the atlantoaxial lateral mass complex, mobile atlantoaxial dislocation, basilar invagination, and periodontoid degenerative tissue mass.