Infectious and Noninfectious Inflammatory Diseases: Wegener Granulomatosis
KEY POINTS
- Wegener granulomatosis should be suspected in destructive or infiltrative processes involving the head and neck region whose morphology mimics neoplasm but biopsies are nonspecific or show a “granulomatous process.”
- Wegener granulomatosis should enter the differential diagnosis when the disease is bilateral and in areas that have a propensity for involvement, especially if there is evidence of sinonasal or nasopharyngeal disease.
- If Wegener granulomatosis is suspected, suggest that a circulating antineutrophil cytoplasmic antibody test be ordered.
- The terms lethal midline granuloma and polymorphic reticuloses, among others, are no longer appropriate, as these diseases are a form of angiocentric lymphoma.
- If for any of the reasons suggested in this chapter the diagnosis of circulating antineutrophil cytoplasmic antibody seems very likely, persist in your opinion—the diagnosis is often difficult to confirm histologically.
ETIOLOGY, PREVALENCE, PATHOLOGIC DIAGNOSIS, AND DISTRIBUTION OF THE DISEASE
Wegener granulomatosis (WG) is a systemic disease of unknown etiology characterized by necrotizing granulomas and vasculitis of the upper and lower respiratory tract, systemic vasculitis, and necrotizing glomerulitis.1 The degree of involvement of each area, in a given patient, is variable. Head and neck manifestations of WG are common at the time of presentation. WG is mainly a disease of white persons occurring in almost all age groups but is infrequent in children and peaks in the 30- to 50-year age bracket.2
In general, WG is a disease that arises primarily in the respiratory tract mucosa and then spreads as an inflammatory, necrotizing vasculitis to other organ systems.3 In the head and neck region, the sinonasal tract (Figs. 17.1–17.3) is the most common site of involvement followed by the nasopharynx (Figs. 17.4 and 17.5). From these sites, it spreads to contiguous sites such as the cavernous sinus, temporal bone, and orbit (Fig. 17.6). Localized presentations of the disease in the head and neck region and elsewhere can go on to more generalized disease.
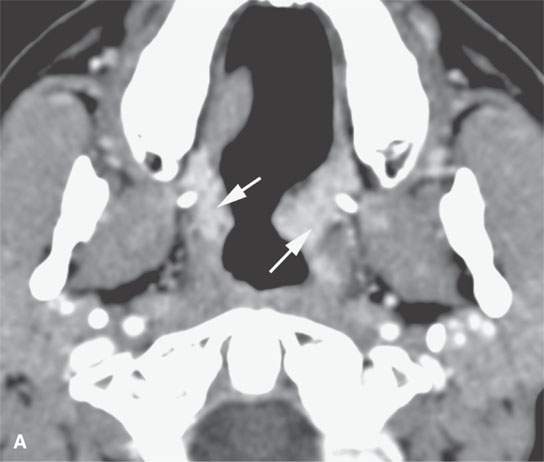
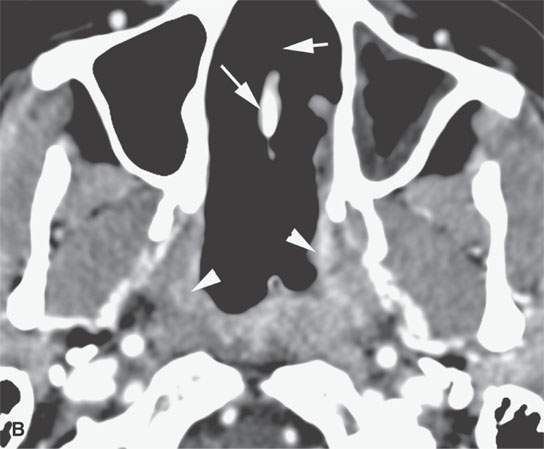
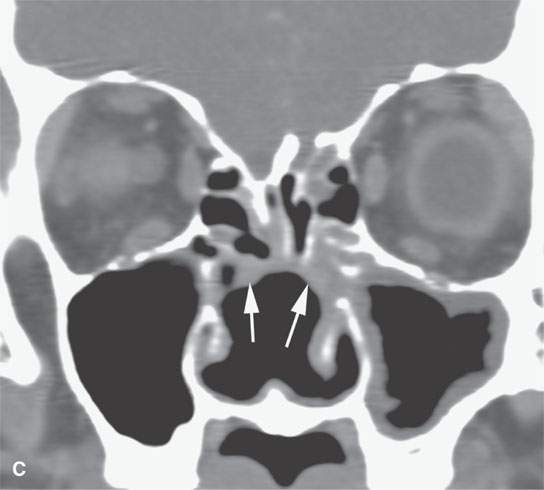
FIGURE 17.1. Contrast-enhanced computed tomography of a patient with new-onset Wegener granulomatosis showing the necrosis of the nasal septum and turbinates (arrows) and residual infiltrating active disease (arrowheads).
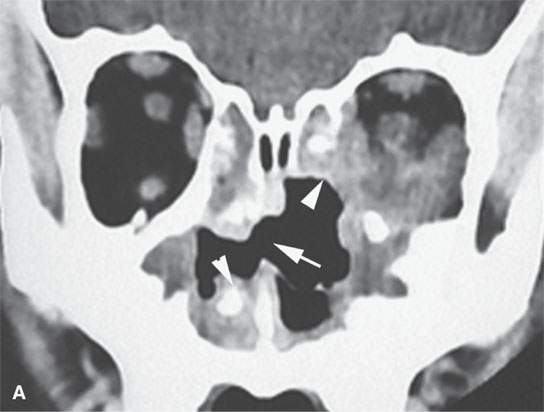
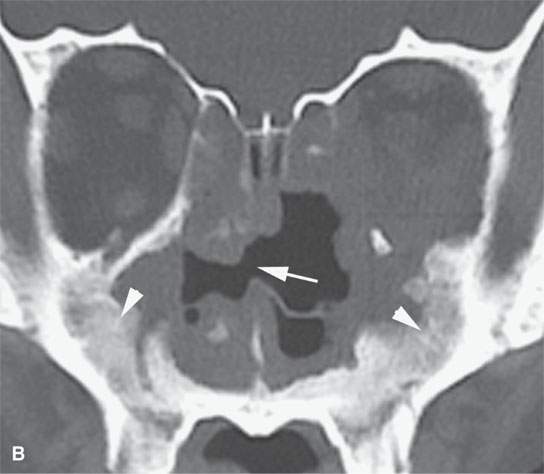
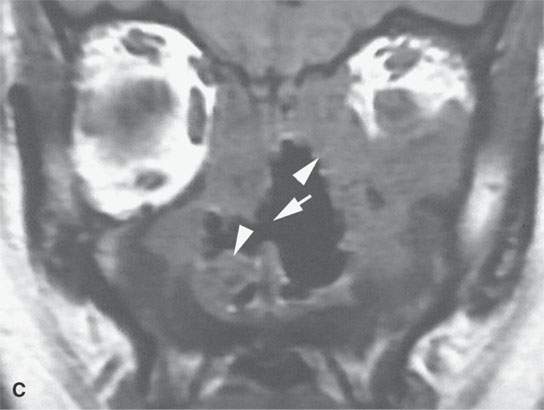
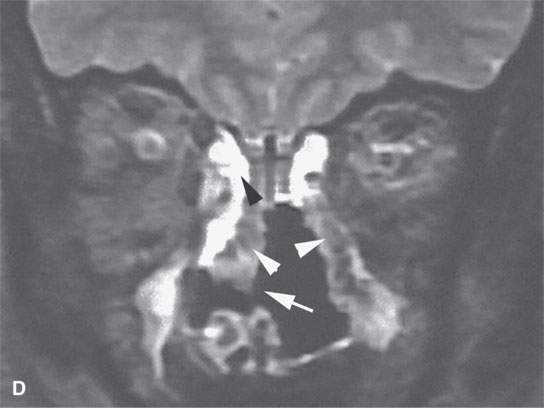
FIGURE 17.2. Contrast-enhanced computed tomography (CT) and magnetic resonance imaging of chronic Wegener granulomatosis showing nasal septal necrosis (arrows). The destructive soft tissue changes (white arrowheads) enhance (arrowheads in A) and can be differentiated from routine sinus inflammation (black arrowhead in D). Bony reactive changes are present but best demonstrated on the CT (white arrowhead in B).
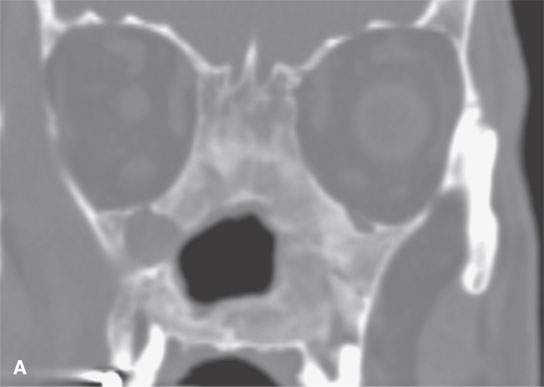
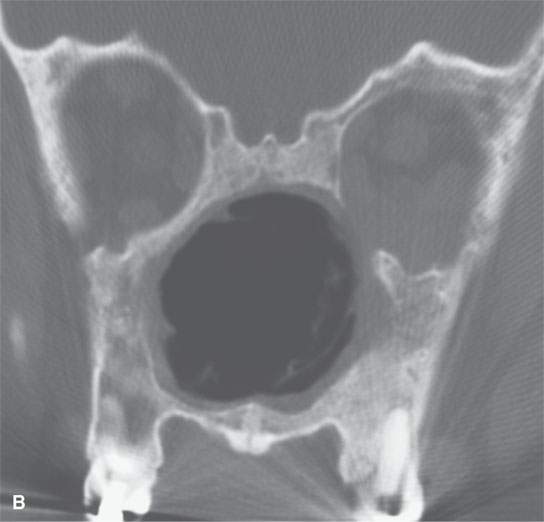
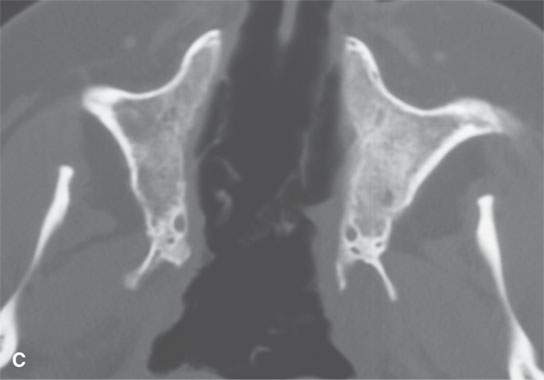
FIGURE 17.3. Computed tomography study in chronic and for the most part “burned-out” Wegener granulomatosis (same patient as in Fig. 17.2 years later) with reactive bone so extensive that it obliterates the sinus and nasal cavities.
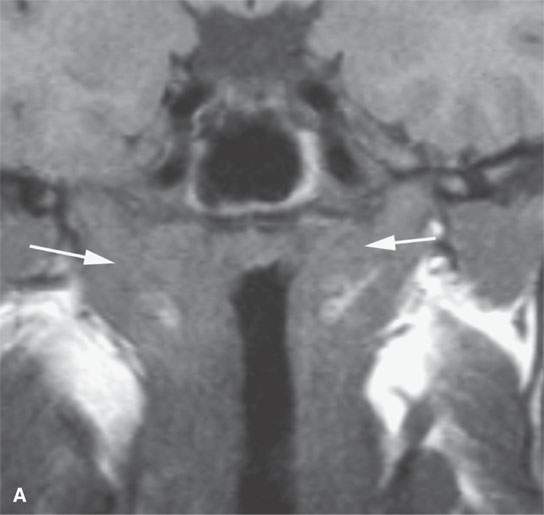
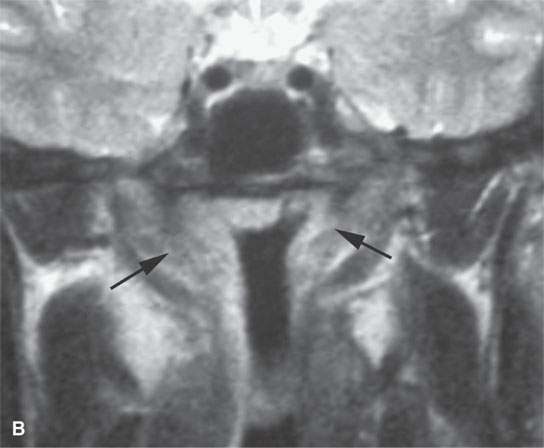
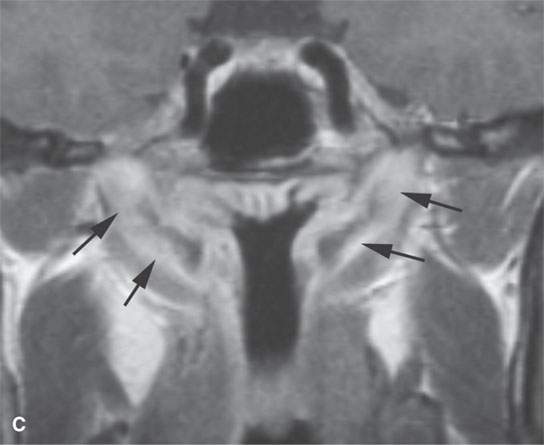
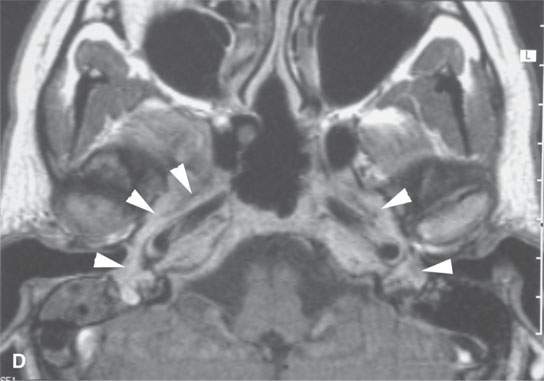
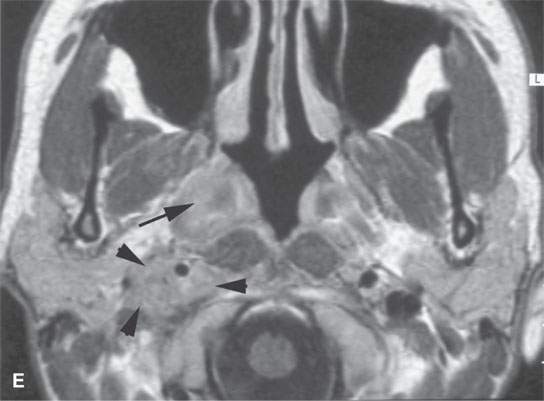
FIGURE 17.4. Contrast-enhanced magnetic resonance in a patient with Wegener granulomatosis. Non–contrast-enhanced T1-weighted (T1W) coronal image (A) shows infiltration of the deep tissue planes of the nasopharynx (arrows). T2-weighted coronal image (B) shows these same areas to be edematous. Contrast-enhanced T1W coronal image (C) shows extensive enhancement along the eustachian tubes (arrows). Axial contrast-enhanced T1W images show disease extending along the eustachian tube to the middle ear on both sides (arrowheads in D), the nasopharyngeal wall (arrow in E), and retrostyloid parapharyngeal space (arrowheads in E).
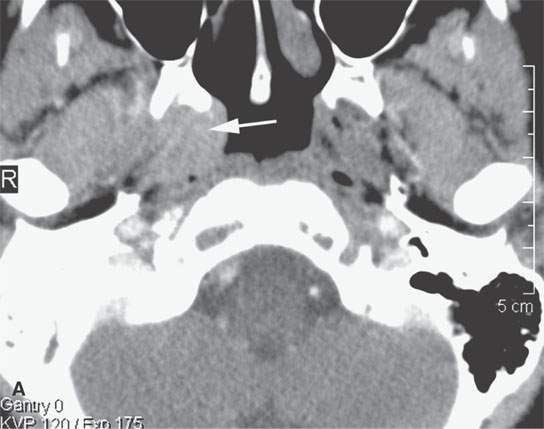
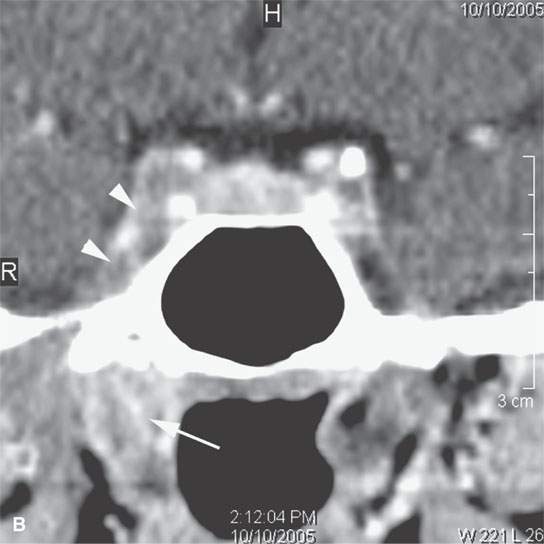
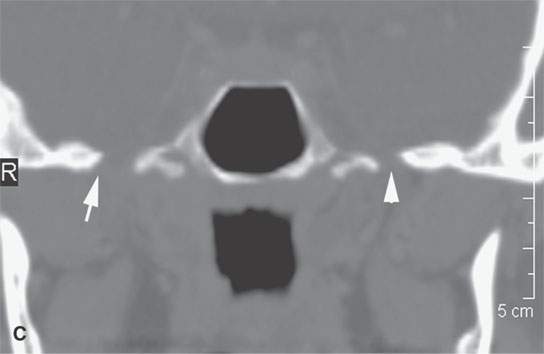
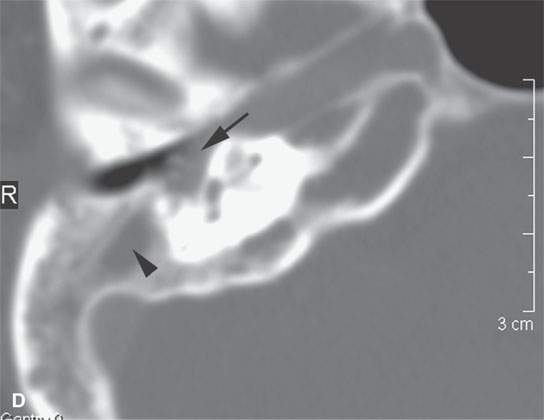
FIGURE 17.5. Contrast-enhanced computed tomography of a patient with Wegener granulomatosis (WG) of the nasopharynx presenting with unilateral chronic right otitis media considered most likely a nasopharyngeal carcinoma, but there was no retropharyngeal or cervical adenopathy. When biopsy returned “inflammatory cells” only, circulating antineutrophil cytoplasmic antibody (c-ANCA) testing was done and WG diagnosed. The patient responded completely to cyclophosphamide. A: There is a minimally enhancing soft tissue mass around the eustachian tube (arrow). B: The infiltrating process (arrow) spreads to the trigeminal cistern and cavernous sinus (arrowheads). C: The skull base is eroded at the foramen ovale on the left (arrow) compared to the normal side (arrowhead). D: The presenting middle ear (arrow) and mastoid disease (arrowhead) is demonstrated. This could be due to obstruction or the disease itself.
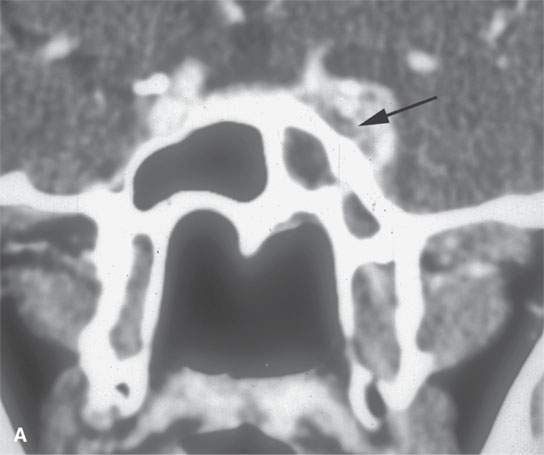
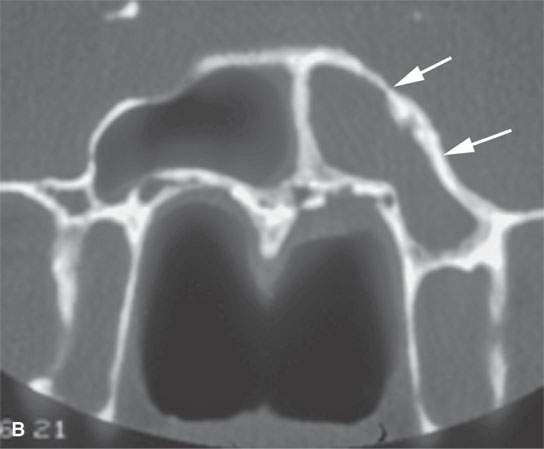
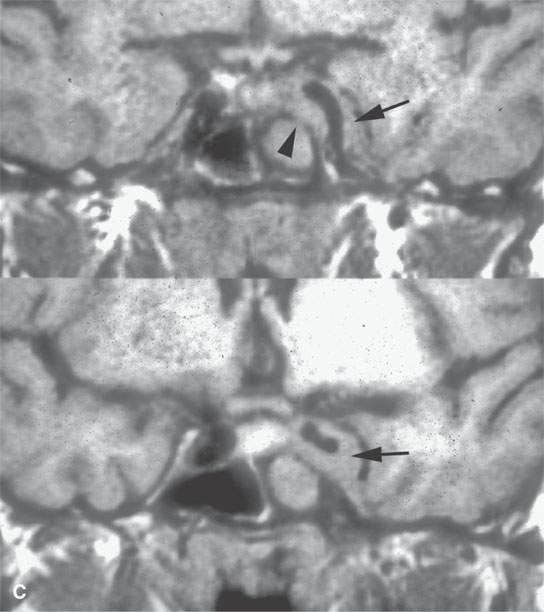
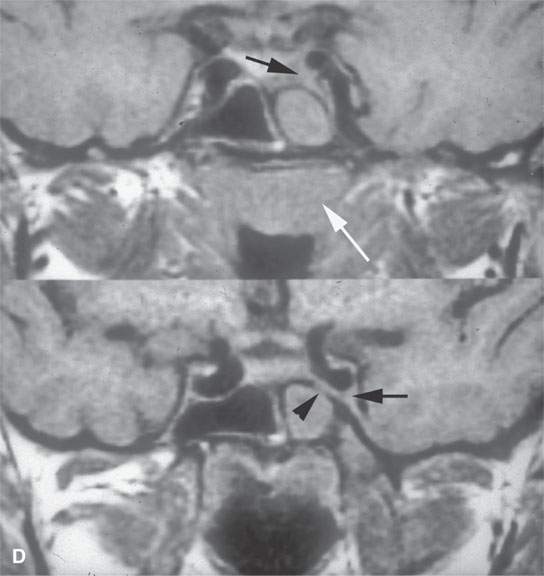
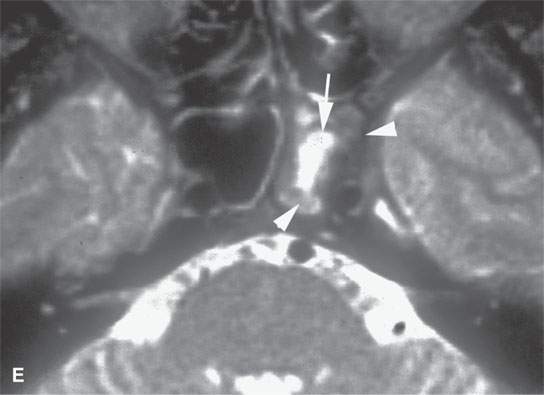
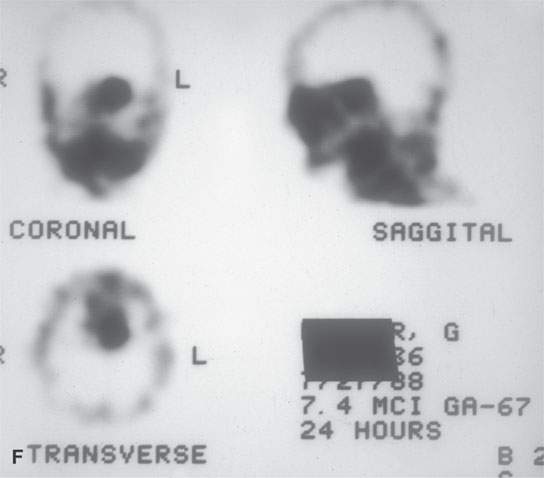
FIGURE 17.6. A patient presenting with ocular motility disorder with likely third and fourth cranial nerve palsies and facial pain on the left. A: Contrast-enhanced computed tomography showing an enhancing mass in the anterior aspect of the cavernous sinus (arrow) and mucosal thickening in the sphenoid sinus. B: The bone of the sphenoid sinus is thickened but not obviously eroded (arrows). C, D: Coronal non–contrast-enhanced T1-weighted images showing the infiltrating mass in the cavernous sinus (arrows) region, suggesting that the bone is infiltrated (arrowheads). In (D), there is a suggestion of nasopharyngeal involvement (white arrow). E: T2-weighted image showing very bright reactive changes centrally in the sinus (arrow) and the darker changes at the periphery and in the cavernous sinus (arrowheads). This image was key to diagnosis since the reactive mucosa had to be stripped by the surgeon before the tissue diagnosed as Wegener granulomatosis could be sampled. F: Gallium scan was positive and used to monitor the response to therapy.
Related posts:
 Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
Preseptal Compartment: Acute and Chronic Infections and Noninfectious Inflammatory Conditions
 Necrotizing (“Malignant”) Otitis Externa
Necrotizing (“Malignant”) Otitis Externa
 Cervicothoracic Junction: Brachial Plexus Trauma
Cervicothoracic Junction: Brachial Plexus Trauma
 Oropharynx: Introduction
Oropharynx: Introduction
 Branchial Apparatus Developmental Anomalies
Branchial Apparatus Developmental Anomalies
 Oral Cavity and Floor of the Mouth: Malignant Tumors
Oral Cavity and Floor of the Mouth: Malignant Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


