Fig. 27.1
Occluded anterior tibial artery
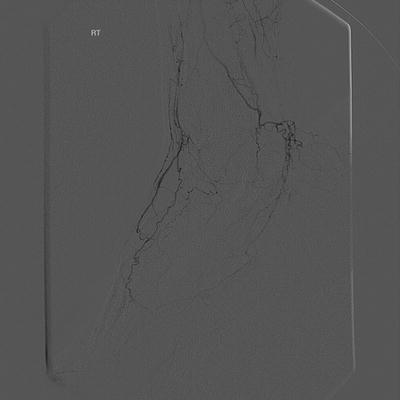
Fig. 27.2
Reconstituted anterior tibial artery at ankle
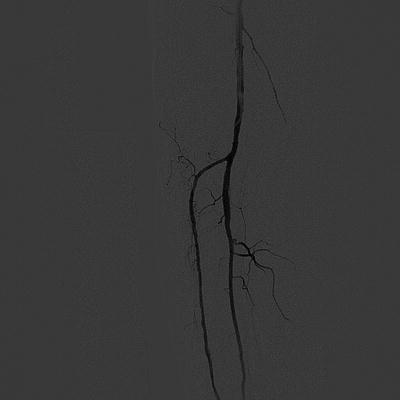
Fig. 27.3
Recanalized anterior tibial artery—proximal
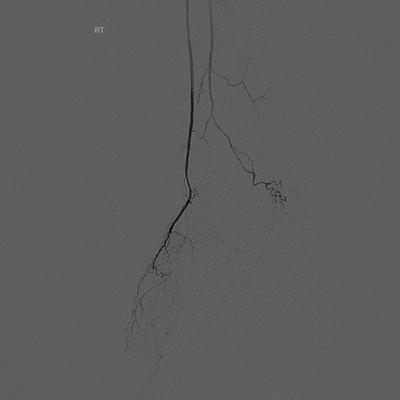
Fig. 27.4
Recanalized anterior tibial artery—distal
4.
Subintimal angioplasty: A hydrophilic angle-tipped guidewire is made to form a loop by its natural tendency to do so when the tip catches on a plaque or when it encounters the occlusion. The guidewire is then used to create a dissection between the intima and the media. The wire/catheter combination is advanced within this plane to bypass the occlusion. The guidewire will naturally tend to break back into the true lumen when it again encounters normal vessel. The newly created false lumen is then angioplastied or stented.
5.
Stenting: Stents have a limited role in the popliteal artery because the flexion of the knee causes metal fatigue and subsequent stent fracture. Some newer stents are more flexible and are licenced for use in the popliteal artery. The small calibre of the crural vessels makes them susceptible to re-occlusion with thrombus or intimal hyperplasia. The use of stents here remains unproven.
6.
Mechanical atherectomy: Mechanical atherectomy devices are available such as the Turbohawk (eV3, Plymouth, MN, USA), which physically removes the artheroma in order to replicate the effect of a surgical endarterectomy. These devices may play a role in recurrent lesions refactory to repreated conventional angioplasty or to treat instent stenosis.
10.2 Pitfalls
Fresh thrombus: A short history or recent sudden deterioration of symptoms should raise suspicion of fresh thrombotic occlusion. This is a critical thing to look for in the preintervention ultrasound. Missing this finding places one at risk of catastrophic embolization with angioplasty. The guidewire will pass through the occlusion very easily. Careful injection of a small volume of contrast produces a characteristic appearance. A suction embolectomy can be attempted, if however unsuccessful angioplasty should be delayed by at least 3 months.
Vasospasm: Very common in small distal vessels. Vasodilators such as GTN (50–250 mcg) or tolazoline (5 mg) can be used, being injected intra-arterially for direct delivery.
Elastic recoil: The vessel fails to remain open despite administering vasodilators and performing repeated prolonged angioplasty. Self-expanding stents are the only method of treating this; however, they have their long-term patency problems as discussed earlier. The subintimal channel is likely to thrombose acutely.
Re-entry failure:




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
