Reporting MR imaging of pelvic floor dysfunction can be made easy if radiologists understand the aim of each MR sequence and what to report in each set of MR images. For an MR imaging report that is critical in decision making for patient management, it is of paramount importance to the radiologist to know what to look for and where to look for it. This article presents a new term, integrated MR analytical approach . A reporting template is included in which all MR findings are presented in a schematic form that can be easily interpreted by clinicians from different subspecialties.
Key points
- •
A diagnostic MR examination of pelvic floor should include MR defecography, dynamic cine MR imaging during straining, and static MR images.
- •
MR defecography is dedicated for detection and grading of pelvic organ prolapse and structural and functional abnormality of the evacuation process.
- •
Dynamic cine MR imaging at maximum straining identifies pelvic floor laxity and quantifies the degree of muscle weakness.
- •
Static MR images are assessed for detection and classification of structural abnormalities.
- •
The integrated MR analytical approach converts static and dynamic MR imaging from 2 separate types of images into an integrated system identifying specific defect in each patient.
Introduction
Many clinicians asserted that the optimal approach to treatment of PFD must be individualized for each patient on the basis of both the symptom complex and the specific anatomical and structural abnormalities. Recently, a new MR imaging analytical approach was devised that integrates data provided by both dynamic (cine) and static MR images, to define the predominant defects of the pelvic support system making it possible to pinpoint the underlying defects in each patient to the clinicians and consequently guides them to tailor treatment to the needs of each patient. This approach provides the necessary scientific evidence on which best clinical practice can be based. The first section of this article, explains why this approach was developed and how to apply it. In addition, to make it easy for radiologists to use this approach and to increase surgeons’ comprehension of the overall findings, a “Data-Reporting System” was created in which all imaging findings are presented in a structured schematic MR imaging reporting template from a purely functional point of view to enhance the radiologists’ interaction with clinicians and bridges the gap between radiology and surgery.
The second section emphasis on what the referring physician needs to know and their requirements to decide on the treatment plan. This section details the vital role of the radiologist in crafting and establishing new aiding tools for the clinician to use in planning reconstructive surgery. “Functional 3-Part Pelvic Supporting Systems Approach”; “Integrated MR Analytical Approach”; “Data-Reporting System”; “Three-axis perineal evaluation (TAPE) Approach”; “Individualized, defect- specific treatment Approach”; “3-D modeling of the predominant pelvic supporting system defect” are the rising stars of the upcoming new horizon in the diagnosis of the complex disorders of the pelvic floor, reducing the risk of surgical failure, dysfunction recurrence, and re-operation.
Mr Imaging Report
In order to achieve an MR imaging report that is critical in decision-making for patient management and /or operative choice, it is of paramount importance to the radiologist to understand clearly the aim of each MR sequences acquired and what to report in each set of the MR images obtained. In other words the radiologist should know “what to look for” and “where to look for it”. ( Fig. 1 ) illustrate this concept in details. ( Figs. 2 and 3 ) provide charts summarizing the essential Kinematic and static imaging protocols for a diagnostic MRI study. In addition the charts specify in which set of the acquired MR images each of the Functional 3-part pelvic supporting system can be assessed.



A clear consensus was reached that the assessment of a MR study of the pelvic floor should include:
- •
Analysis of the MR Defecography for detection and grading of pelvic organ prolapse and functional abnormality of the evacuation process.
- •
Assessment of the Dynamic cine MR images at maximum straining to identify pelvic floor laxity and quantifies the degree of muscle weakness.
- •
Analysis of static MR images for detection and classification of structural abnormalities.
- •
Both dynamic and static MR imaging findings as well as the results of the metric measurements should be reported in a structured MR reporting scheme1 ( Box 1 ).
Box 1
Checklist for the recommended MR imaging reporting scheme
Data from [El Sayed RF, Alt CD, Maccioni F, Meissnitzer M, Masselli G, Manganaro L, Vinci V, Weishaupt D. Magnetic resonance imaging of pelvic floor dysfunction – joint recommendations of the ESUR and ESGAR Pelvic Floor Working Group. On Behalf of ESUR and ESGAR Pelvic Floor Working Group . European Radiology,2017; 27(5):2067–2085. 10.1007/s00330-016-4471-7 ].
A. Measurements
- 1.
Basic measurements for all compartments
- •
Determine PCL.
- •
Determine organ-specific reference points.
- •
Measure the descent of reference points below the PCL.
- •
- 2.
Measurements for posterior compartment
Measure the bulging of the anterior rectal wall during maximum straining phase and evacuation phase.
Measure the ARA at rest, squeezing phase, straining phase and evacuation phase.
B. Reporting
- 1.
Basic reporting for all compartments
- •
Report values above the PCL as negative and below as positive.
- •
Report pelvic organ mobility.
- •
- 2.
Reporting for anterior compartment
- •
Report loss of urine at straining phase.
- •
Report urethral mobility at straining phase.
- •
- 3.
Reporting for middle compartment
- •
Report uterine descent.
- •
Report the content of a present enterocele.
- •
- 4.
Reporting for posterior compartment
- •
Report presence of a rectal intussusception.
- •
Evaluate time-effective rectal evacuation.
- •
Point out the change of ARA.
- •
C. Grading
- 1.
Anterior compartment
- •
Use the rule-of-3 grading for cystocele.
- •
Report cystocele as pathologic starting from °II.
- •
- 2.
Middle compartment
- •
Use the rule-of-3 grading for uterine prolapse and enteroceles.
- •
Report POP as pathologic starting from °II.
- •
- 3.
Posterior compartment
- •
Use the rule-of-2 grading for rectoceles.
- •
Report a rectocele as pathologic starting from °II.
- •
Use the grading for ARJ starting at 3 cm below the PCL.
- •
Analysis of MR Defecography
Dynamic MR imaging examination of pelvic floor are reported in a standardized scheme in all patients of pelvic floor dysfunction, whether the patient’s main complaint is related to one or multiple compartment or whether the patients is being referred from urogynecology and/or coloproctology.
Measurements during evacuation recognize and grade the extent of POP, in addition to any structural or functional abnormalities of the evacuation process in obstructed defecation ( Fig. 4 ).

Basic measurements for all compartments
- •
The pubococcygeal line (PCL), drawn on sagittal plane from the inferior aspect of the pubic symphysis to the last coccygeal joint, is recommended as reference line to measure POP.
- •
After defining the PCL, the distance from each reference point is measured perpendicularly to the PCL during evacuation.
- ▪
In the anterior compartment, the organ-specific reference point is the most inferior aspect of the bladder base.
- ▪
In the middle compartment, the reference point is the anterior cervical lip (most distal edge of the cervix) or the vaginal vault after hysterectomy.
- ▪
In the posterior compartment, the reference point is the anorectal junction (ARJ).
- ▪
Measured values above the reference line have a minus sign and values below a plus sign. ,
- ▪
- •
Stress urinary incontinence (SUI) is recorded when loss of urine through the urethra is visualized at maximum straining. The absence of urine loss during MR imaging, however, does not preclude the patient experiencing symptoms.
Grading of pelvic organ prolapse in anterior and middle compartments
Anterior compartments
- •
It has been reported that the pelvic floor may descend and widen up to 2 cm during abdominal pressure. Consequently, the pelvic organs follow the movement of the pelvic floor inferiorly but without protrusion through their respective hiatuses.
- •
The rule of 3 is the recommended grading system in the anterior and middle compartments starting at 1 cm below the PCL , (see Box 1 ).
- •
Urethrocele
- ○
Urethrocele is the prolapse of the female urethra into the vagina.
- ○
It often occurs with cystoceles; in this case, the term used is cystourethrocele .
- ○
- •
Cystocele
- ○
The bladder base, in particular, may descend up to 1 cm below the PCL during straining in continent women and should not be stated as a cystocele.
- ○
Grading of cystocele
- ▪
Grade 0: up to +1 cm below PCL
- ▪
Grade 1: +1 to +3 cm below PCL
- ▪
Grade 2: +3 to +6 cm below PCL
- ▪
Grade 3: greater than + 6 cm below PCL
- ▪
- ○
Middle compartments
- •
True prolapse is complete organ eversion; however, the term is commonly used to generically describe any degree of pelvic organ descent.
Classification
- •
Anterior vaginal wall prolapse ,
- ○
Cystocele
- ○
Uterine prolapse
- ○
- •
Posterior vaginal wall prolapse
- ○
Enterocele
- ○
Rectocele
- ○
- •
Vaginal vault prolapse
- ○
Vaginal opacification with sterile lubricating gel to enhance visualization of the vaginal apex is strongly advised, if not mandatory.
- ○
- •
Peritoniocele
- ○
A peritoneocele is a protrusion of the peritoneum between the rectum and vagina that does not contain any abdominal viscera.
- ○
If a peritoniocele is present, the report should include the content of the peritoneal sac, because clinical examination alone may have shortcomings in identifying the content.
- ○
- •
Grades of pelvic organ prolapse
- •
Grade 0: above PCL
- •
Grade 1; mild: descent less than 3 cm below PCL
- •
Grade 2; moderate: descent 3 cm to 6 cm below PCL
- •
Grade 3; severe: descent greater than 6 cm below PCL
- •
Grade 4: cases of complete uterine prolapse
- •
Posterior compartment
Constipation and obstructed defecation
Definitions and general considerations
- •
Constipation describes a symptom, not clinical a sign, and is particularly subjective, meaning different things to different people.
- •
There is considerable individual variation in defining constipation:
- ○
Some patients concentrate on bowel frequency.
- ○
Others are more concerned about ease of defecation and stool size/consistency.
- ○
- •
Satisfactory definition of constipation must include both infrequent defecation and difficult evacuation.
- ○
Infrequent defecation
- ▪
Usually defined as less than 3 bowel movements per week
- ▪
Most likely associated with slow transit time
- ▪
- ○
Difficult evacuation
- ▪
Straining at stool is considered abnormal if it occurs for greater than 25% of time spent in lavatory
- ▪
Indicates obstructed defecation
- ▪
- ○
Chronic constipation
- ▪
Very common
- ▪
Estimated that 1 in 5 healthy, middle-aged adults have symptoms suggesting functional constipation
- ▪
- ○
Obstructed defecation
Outlet obstruction is due either to structural or functional underlying pathology.
Structural pathology
- 1.
Rectocele
- •
A rectocele is diagnosed as an anterior rectal wall bulge and it is measured during maximum straining and evacuation.
- •
Typically, a line drawn through the anterior wall of the anal canal is extended upward, and a rectal bulge of greater than 2 cm anterior to this line is described as a rectocele.
- •
Due to the different classification of the pathology in the posterior compartment, it has different grading systems from the anterior and middle compartments.
- •
The rule of 2 is recommended for grading the anterior rectal wall bulge in rectoceles (see Box 1 ).
- ○
Grading
- ▪
Grade 0: no outpouching
- ▪
Grade 1: outpouching up to 2 cm
- ▪
Grade 2: outpouching between 2 cm and 4 cm
- ▪
Grade 3: outpouching greater than 4 cm. ,
- ▪
- ○
Anterior rectal wall bulge should be reported as pathological if it is grade II and higher, because grade I rectocele can be observed in approximately 78% to 99% of parous women.
- ○
- •
- 2.
Descending perineum syndrome (pelvic floor descent)
- •
Defined as descent of ARJ greater than 3 cm below the PCL (see Fig. 4 B)
- •
ARJ is defined by posterior impression of puborectalis muscle at most cranial extent of anal canal.
- •
Usually generalized process with associated abnormal descent of middle and anterior pelvic floor compartments
- •
Often seen in combination with perineal ballooning, rectocele, intussusception, and impaired evacuation
- ○
Grading
- ▪
Grade I: between 3 cm and 5 cm below the PCL
- ▪
Grade II: with at least 5 cm ,
- ▪
- ○
- •
- 3.
Intussusception and rectal prolapse
- •
Rectal prolapse is a circumferential full-thickness intussusception of the rectal wall with protrusion beyond the anal verge.
- •
Intussusception (internal rectal prolapse) is full-thickness prolapse of rectum (see Fig. 4 D) that does not protrude through the anus; it could be either
- a.
Intrarectal intussusceptions that are confined to rectal ampulla
- b.
Intra-anal intussusception that extends into anal canal
- a.
- •
Precautions during MR imaging defecography
- ○
Intussusception occurs only when rectum collapses during evacuation; therefore, the end of evacuation phase is important to identify intussusception (see Fig. 4 D).
- ○
Small intussusceptions of the rectal wall are considered normal findings during defecation, observed in approximately 80% of healthy subjects. ,
- ○
- •
Functional pathology
- 1.
Dyskinetic puborectalis
- •
Also called s pastic pelvic floor syndrome or anismus
- •
Defined as involuntary contraction of the puborectalis muscle with failure to relax, which prevents normal rectal evacuation.
- •
Not an uncommon cause of obstructed defecation and frequently overlooked at imaging
- •
Highly likely that many surgical failures occur in patients treated for rectocele because underlying anismus was not recognized
- •
Diagnostic criteria
- ○
Normal anorectal angle (ARA)
- ▪
The ARA is the angle enclosed between a line plotted along the posterior rectal wall and the second line is plotted along the central axis of the anal canal on sagittal plane at rest, squeezing and maximum straining.
- ▪
The change of the ARA during evacuation compared with rest expresses the functioning of the puborectal muscle; in particular, the ARA should sharpen during squeezing and should become more obtuse during straining and evacuation.
- ▪
It is recommended to report that the ARA showed the normal changes at different maneuvers rather than the absolute value of the ARA angle, because the literature presents a widespread of normal reference values.
- ▪
- ○
MR findings in spastic pelvic floor syndrome
- ▪
Failure of ARA to open
- ▪
Persistent or exaggerated puborectal impression on posterior aspect of ARJ
- ▪
Lack of descent of pelvic floor during defecation
- ▪
Long interval between opening of anal canal and start of defecation
- ▪
Most pertinent finding for diagnosis of anismus is prolonged and incomplete evacuation; using 120 mL of rectal contrast, evacuation times of more than 30 seconds accurately predict this functional disorder ( Fig. 5 A ). , , ,

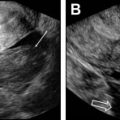
Fig. 5
MR defecography, functional outlet obstruction. ( A ) Paradoxic contraction of puborectalis during defecation ( red arrow ) and relaxed anal sphincter. ( B ) Nonrelaxing or spastic anal sphincter evident by anal canal diameter measuring less than 15 mm ( red arrows ). Note total obliteration of the posterior ARA indicating relaxed puborectalis. There is also grade 3 anterior rectocele. B, bladder; C, cervix; Rec, rectum.
- ▪
- ○
- •
- 2.
Spastic anal sphincter contraction
- •
Also known as spasmodic contraction of anal sphincter or anal sphincter achalasia
- •
Under normal circumstances, expansion of rectum or rectosigmoid causes internal anal sphincter (IAS) reflex relaxation.
- •
Patients usually present with painless constipation associated with dry stools.
- •
Resting anal pressure is significantly higher than normal on manometry.
- •
MR findings
- ○
Anal canal is not open with dilatation of rectum.
- ○
Resting dilated rectum or even giant rectum
- ○
MR defecography is mandatory to show rate of evacuation (see Fig. 5 B).
- ○
Static MR should show normal anal sphincter muscle complex to exclude IAS hypertrophy.
- ○
- •
Structural and functional pathology
Solitary rectal ulcer syndrome
- •
Well-recognized diagnosis that describes a combination of rectal prolapse and functional pelvic floor abnormality
- •
MR findings
- ○
Usually the imaging findings in these patients are a combination of rectal prolapse and puborectalis dyskinesia.
- ○
- •
Pathogenesis: incompletely understood
- ○
Prolapsed rectal mucosa is forced downward due to pressures generated during defecation and is compressed by force of paradoxic puborectalis contraction, leading to mucosal ischemia and ulceration secondary to repeated straining.
- ○
Proctoscopy usually reveals rectal inflammationand ulceration and is accompanied by specific histopathological changes within prolapsing mucosa.
- ○
- •
Analysis of Dynamic Cine MR Images at Maximum Straining
- •
Analysis of the dynamic MR images is dedicated to supportive measurements.
- ○
These are 5 measurements of supporting structures measured in the 3 orthogonal plane ( Fig. 6 ).
- ○