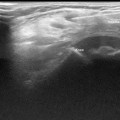
Fig. 11.1
Transabdominal ultrasound of cystic abdominal mass demonstrating an anechoic, irregularly shaped cystic lesion at midline located anterior to the SMA and SMV and inferior to the pancreas. Lesion measured 8 × 3 cm and was compressible (arrows). Surgery demonstrated this to be a mesenteric cyst. SMA superior mesenteric artery, SMV superior mesenteric vein
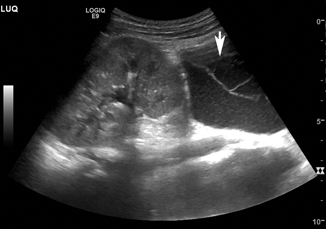
Fig. 11.2
Transabdominal ultrasound of cystic retroperitoneal mass (arrows) demonstrating multicompartmental collections filled with fluid adjacent to the kidney. Lesion was noted by CT scan to be consistent with retroperitoneal lymphatic malformation
Pseudocyst
A meconium pseudocyst forms secondary to an intestinal perforation during fetal life. The inflammatory reaction from this chemical peritonitis causes the perforation to seal, and the meconium that was released into the peritoneal cavity is walled off into a pseudocyst. Ultrasound examination will demonstrate a cystic mass with heterogeneous echogenicity [3]. There may also be calcifications present, causing shadowing of the cyst, which can sometimes be seen on plain radiographs.
Urachal Cyst
Urachal cysts are most frequently seen in infants and young children. They arise when the urachus obliterates at the umbilicus and the bladder, but not in between. Most urachal cysts remain asymptomatic, but some may present as a palpable abdominal mass, an infection of the cyst, or as symptoms from compression of adjacent structures. Ultrasound demonstrates a hypoechoic, thick-walled cystic structure, often just superior to the bladder wall. [18]
Pelvis
Uterus/Ovaries
Ovarian Cysts
Ovarian cysts are common in the neonatal period, likely secondary to in utero hormone exposure [22]. They may be diagnosed on prenatal ultrasound, or present symptomatically with pain, abdominal distension, or fever—usually as a result of torsion or hemorrhage. Sonography of ovarian cysts (Fig. 11.3) usually demonstrates a simple cyst with no internal echoes, and a thin wall. If there has been torsion or hemorrhage, the inner part of the cyst will contain echogenic debris. Doppler ultrasound may differentiate a hemorrhagic cyst from other ovarian neoplasms, as the latter would demonstrate internal flow. Ovarian torsion may be demonstrated by the whirlpool sign , which represents the twisted pedicle of the ovary [14]. Doppler flow to the ovarian parenchyma may be absent (Fig. 11.4) but this absence should not be used to rule out torsion since some studies have demonstrated Doppler flow in up to 50 % of torsed ovaries. Simple cysts that are less than 4 cm and have no solid component may be monitored with serial ultrasound examinations [16]. Removal of cysts is generally reserved for large, symptomatic, or torsed cysts.

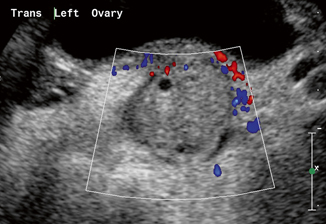
Fig. 11.3
Transabdominal ultrasound of the pelvis demonstrating an anechoic cyst near an ovary measuring 11.6 × 4.7 cm. Laparoscopic examination demonstrated this to be a paratubular cyst, which was excised
Fig. 11.4
Transabdominal ultrasound of the pelvis demonstrating an enlarged left ovary with small peripherally displaced follicles and heterogenous stromal echogenicity. Ovary measure 3 × 2 × 4 cm. Color and spectral Doppler demonstrated no arterial or venous flow. Laparoscopic detorsion was performed immediately thereafter
Solid Masses
Retroperitoneal
Kidney
Wilms’ Tumor
Wilms’ tumor is the most common renal malignancy in childhood. The majority of patients are between 1 and 5 years of age, and present with an asymptomatic abdominal mass. The diagnosis of Wilms’ tumor is associated with various conditions, including Beckwith–Weidemann syndrome, sporadic aniridia, Drash syndrome, and hemihypertrophy [8]. In fact, it is recommended that patients with either Beckwith–Weidemann or hemihypertrophy should be screened with an abdominal ultrasound every few months due to their increased risk of Wilms’ tumor. Ultrasound examination of Wilms’ tumor will reveal an echogenic, solid mass within the kidney that may contain some cystic areas (Fig. 11.5). Increased tumor vascularity will be noted with Doppler sonography. Careful attention should be paid to the extent of tumor involvement in regard to the perinephric space, inferior vena cava (IVC) (Fig. 11.6), and rarely, the right atrium. Peritoneal lymphadenopathy may also be seen. Further staging via a CT scan is recommended following the diagnosis of Wilms’ tumor in order to determine tumor rupture, contralateral kidney involvement, and/or lung involvement.

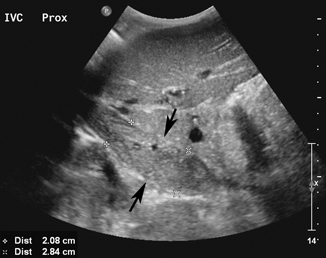
Fig. 11.5
Transabdominal ultrasound of a diffusely enlarged and heterogenous left kidney (arrows)
Fig. 11.6
Transabdominal ultrasound of patient with a renal tumor and associated large IVC tumor thrombus (arrows). Patient was treated with preoperative chemotherapy and subsequently underwent nephrectomy with tumor thrombectomy
Congenital Mesoblastic Nephroma
CMN is the most common renal neoplasm of infancy, with 85 % of CMNs diagnosed prior to 6 months of age [15]. Presentation is often with a palpable abdominal mass and, occasionally, with a paraneoplastic syndrome such as hypertension or hypercalcemia. Sonography demonstrates a large, solid renal mass with heterogeneous echogenicity. Color Doppler will demonstrate internal flow. Often, there is a central area of necrosis that is hypoechoic in nature. Though this tumor may extend beyond the renal capsule, involvement of the renal vein is uncommon. CMN may be similar in appearance to Wilms’ tumor, but is differentiated based on age of presentation given that Wilms’ tumor is rarely seen in neonates.
Adrenal Gland
Neuroblastoma
Neuroblastomas are tumors derived from neural crest cells, and have an incidence of 1:10,000 live births in the USA. Advances in prenatal ultrasound have increased the prenatal detection of neuroblastoma. Furthermore, screening ultrasound in early neonates may also reveal adrenal masses, such that 30 % of neuroblastomas may be diagnosed in the neonatal period [9]. It was unknown if some of the early detection of these lesions was merely a result of increased sensitivity of the screening ultrasound, and therefore not clinically significant. Indeed, ultrasound screening performed in Japan and Quebec has demonstrated that many of these small lesions will regress spontaneously [12]. Such screening has been discontinued as the lesions detected early were low-staged tumors and the program did not alter the overall survival in the entire cohort. Ultrasound findings of neuroblastoma tend to vary with the stage of the tumor. In lower-stage tumors, ultrasound reveals a homogeneous or slightly heterogeneous solid mass that replaces the adrenal gland . At more advanced stages, this mass tends to have a much more heterogeneous echotexture, increased vascularity, and multiple intralesional calcifications [1]. All patients with neuroblastoma should receive a staging CT and a metaiodobenzylguanidine (MIBG) scan to determine the extent of involvement. Treatment is based on tumor stage, and certain neuroblastomas (4S) may be followed with serial ultrasound or CT to determine regression and need for surgery.
Abdominal
Liver
Infantile Hepatic Hemangioma
Hemangioma is the most common benign liver mass in infants and children, with a peak presentation between 3 and 6 months of age [5]. Presenting signs and symptoms range from a palpable abdominal mass to congestive heart failure and thrombocytopenia as a result of Kasabach–Merritt syndrome. Sonography will demonstrate a complex, solid mass with heterogeneous echotexture (Fig. 11.7) and robust Doppler flow. Infantile hemangiomas typically increase in size until 9–10 months of age, and then slowly involute [6]. Medical therapies for those that do not involute spontaneously include the use of propranolol and corticosteroids. Embolization or surgical removal is reserved for those that do not involute with medical therapy, or for patients with severe complications.
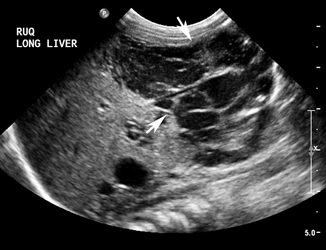
Fig. 11.7
Transabdominal ultrasound of infant with large right hepatic mass with cystic spaces and increased blood flow. Patient also had congestive heart failure. Image and presentation is typical of a large, symptomatic hepatic hemangioma. The child was started on oral propranolol and has had significant improvement in symptoms and resolution of the liver mass
Hepatoblastoma
Malignant tumors comprise the majority of hepatic masses in children, with the most common tumor being hepatoblastoma [5]. Hepatoblastoma typically presents in children between the ages of one and three as a palpable abdominal mass. Initial ultrasound evaluation typically shows a well-defined, heterogeneous tumor often with cystic areas caused by necrosis and calcifications. Use of a high-frequency (> 7 MHz) linear transducer will aid in the evaluation of portal and hepatic venous involvement. The tumor may invade the venous system, or cause the formation of an echogenic tumor thrombus within the lumen of the vessels. The intraluminal material may be examined with Doppler sonography, and if there is arterial flow within the intraluminal material, venous invasion by the tumor is likely.
Hepatocellular Carcinoma
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


