Intracranial pressure (ICP) is the pressure within the intracranial space. Intracranial hypotension is a clinical syndrome in which low cerebrospinal fluid volume (CSF) results in orthostatic headache. Severe cases can result in nausea, vomiting, photophobia, and, rarely, decreased level of consciousness and coma. CSF opening pressure can be within the normal range in spontaneous intracranial hypotension. Imaging tests therefore play a key and decisive role in the diagnosis, as well as treatment, of intracranial hypotension. Intracranial hypertension occurs in a chronic form known as idiopathic intracranial hypertension, as well as in a large variety of neurologic and systemic disorders. Symptoms include headache, nausea and vomiting, blurred vision, and in severe cases, altered level of consciousness that can progress to coma and death. Direct measurements of CSF pressure through lumbar puncture (in idiopathic intracranial hypotension) or invasive ICP monitoring (in acute intracranial hypertension) are the key diagnostic tests. Imaging is used primarily to determine treatable causes of increased ICP, to assess for impending brain herniation, and to evaluate ventricular size.
Intracranial pressure
Intracranial pressure (ICP) is the pressure within the intracranial space. In the steady state, pressure within the brain parenchyma and intracranial extra-axial spaces are equal. Normal values of ICP are 5 to 15 mm Hg (6–20 cm H 2 O) in adults and older children (ages 8 years and older) in the supine position, 1 to 7 mm Hg (1–10 cm H 2 O) in younger children, and up to 18 mm Hg (25 cm H 2 O) in obese patients. ICP increases with Valsalva maneuver, and falls below atmospheric pressure in the standing position. In the lateral decubitus position with lower extremities and neck in neutral position, ICP is approximately equal to intraspinal pressure, and can be estimated by measurement of the cerebrospinal fluid (CSF) opening pressure at lumbar puncture.
Intracranial hypotension is a clinical syndrome in which low CSF volume results in orthostatic headache. Severe cases can result in nausea, vomiting, photophobia, and, rarely, decreased level of consciousness and coma. CSF opening pressures of less than 6 cm H 2 O are typical in intracranial hypotension. However, because CSF opening pressure can be within the normal range in spontaneous (or primary) intracranial hypotension (SIH), imaging tests frequently play a key and decisive role in its diagnosis.
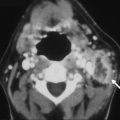
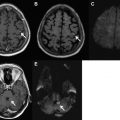
Intracranial hypertension occurs in a chronic form known as idiopathic intracranial hypertension (IIH), as well as in a large variety of neurologic and systemic disorders, including intracranial mass, traumatic brain injury, ischemic or hemorrhagic stroke, hydrocephalus, dural sinus thrombosis, dural arteriovenous fistula, and diffuse cerebral edema such as in liver failure. ICP in the range of 20 to 30 mm Hg is considered mildly increased, whereas ICP persistently exceeding 40 mm Hg is severe and life threatening. Symptoms of intracranial hypertension include headache, nausea and vomiting, blurred vision, and in severe cases, altered level of consciousness and death. Direct measurements of CSF pressure through lumbar puncture (in IIH) or invasive ICP monitoring (in acute intracranial hypertension) are essential diagnostic tests. Imaging is used primarily to determine causes of increased ICP, to assess for impending brain herniation, and to evaluate ventricular size.
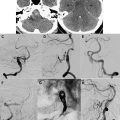
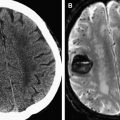
The Monro-Kellie doctrine describes the relationship among volumes and pressures in the intracranial space, and is relevant to both intracranial hypotension and intracranial hypertension clinical syndromes. It is based on the principle that, within the fixed volume of the intracranial and intraspinal spaces, the total volume of CSF, brain and spinal cord, and intracranial and intraspinal blood volume remains approximately constant. A change in the volume of any one of the compartments is offset by compensatory changes in the other two compartments. For example, in intracranial hypotension, a reduction of CSF volume results in compensatory enlargement of intracranial venous and arterial structures. If expansion of the cerebral vascular volume does not offset the loss of CSF, formation of subdural collections and subdural hematomas may occur. In intracranial hypertension caused by space-occupying mass lesions, the Monro-Kellie doctrine may be manifested by effacement of cerebral sulci and brain herniation.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


