KEY POINTS
Depending on geographic factors, cytomegalovirus (CMV) and toxoplasmosis are the more frequent intrauterine infections (IUIs).
The pattern of brain involvement in CMV-IUI may range from minimal (small periventricular cysts, intrathalamic vasculopathy) to severe damage (brain atrophy, malformations of cortical development, and hemorrhages).
The prognosis is usually poor in the presence of intracranial findings.
Infected fetuses without brain findings are generally asymptomatic at birth but may develop sensorineural deafness.
The fetus may become infected with a variety of organisms through transplacental passage or as a result of an ascending infection. In some patients, the infection may involve the central nervous system (CNS), causing lesions in different areas and grades of severity (Table 9–1).
| Pathogen | CNS involvement | Reported in | Ventriculomegaly | Abnormal PVWM | Calcifications | Microcephaly | Others |
|---|---|---|---|---|---|---|---|
| CMV | Common | Fetus, infant | Common | Common | Frequent | Frequent | MCD, CC, cerebellum, hemorrhage |
| Toxoplasma | Common | Fetus, infant | Common | Rare | Common | Rare | Hydranencephaly |
| Rubella | Common | Infant | Rare | Common | Common | Common | – |
| Varicella zoster | Extremely rare | Fetus, infant | Rare | – | Rare | Rare | Encephalitis, cerebellum, MCD |
| Herpes simplex | Extremely rare | Fetus, infant | Common | Common | Rare | Rare | Encephalitis |
| Parvovirus B19 | Extremely rare | Fetus, infant | Rare | – | – | – | Hemorrhage, stroke, MCD |
| LCMV | Common | Fetus, infant | Common | Rare | Common | – | – |
| West Nile virus | Extremely rare | Fetus, infant | – | Rare | – | – | Meningitis, encephalitis |
| Syphilis | Extremely rare | Fetus, infant | Rare | Rare | – | Rare | MCD |
| Trypanosoma | Extremely rare | Fetus, infant | – | – | – | – | Meningoencephalitis |
Cytomegalovirus (CMV) and Toxoplasma gondii are the most common pathogens affecting the brain. Other organisms that may infect the developing fetal brain are rubella virus,1 varicella zoster virus,2 herpes simplex virus,3,4 parvovirus B19,5,6 lymphocytic choriomeningitis virus,7 West Nile virus,8 Treponema pallidum,9 Trypanosoma cruzi,10 and the nematode filarial.11 This chapter reviews each of these sources of infection.
Cytomegalovirus (CMV) is a large DNA virus with a wide infectious clinical spectrum ranging from subclinical to severe multisystem involvement. CMV is transmitted by person-to-person contact. Following maternal infection, it may be transmitted through the placenta to the fetus.
Herpesvirus 5, cytomegalic inclusion disease
Following the almost complete disappearance of congenital rubella after the introduction of widespread immunization programs, CMV infection has become the most common infection affecting the developing fetus.
The prevalence of CMV-seropositive pregnant women or at reproductive age ranges from > 99% in Turkey12 to between 43.6% and 57.2% in France13 and England,14 respectively.
A meta-analysis study of 27 culture-based universal study groups found a birth prevalence of congenital CMV of 0.64% (95% CI: 0.60–0.69%).15 The same study found that from 954 infants identified with congenital CMV infection, only 103 (11%) were considered symptomatic.15 A primary infection during pregnancy carries a significantly higher risk of fetal transmission than a recurrent infection (32.3% vs 1.4%).15
Maternal viremia, placental infection, and hematogenous dissemination to the fetus are the most likely sequence of events leading to congenital CMV infection.16 During the viremic phase, the virus circulates and disseminates, carried by leukocytes. The exact way in which CMV infects the placenta is not clearly understood, but once it reaches the fetal compartment, hematogenous dissemination ensues.16 A direct effect on placental development causing placental insufficiency has been described as a possible factor in the pathogenesis of fetal disease.17 CMV may also act as a teratogen, producing chromosomal injury or altering modulation of developmental gene expression.18
CMV infection is caused by a large double-stranded DNA herpesvirus. Geneotypically different CMV strains have been reported.19 Preconceptional immunity against CMV provides only partial protection against intrauterine transmission of the virus, as reinfection with a different strain of CMV may lead to intrauterine transmission and symptomatic congenital infection.20
Intrauterine CMV infection frequently affects the fetal brain; the motif of this predilection is not clear, and the cellular targets not well defined. The presence of intracellular inclusion bodies in the brain (Figure 9–1) is considered diagnostic of CMV infection, but there are almost no histologic data regarding the type of cells affected.21 From human and animal cell line cultures, it seems that neural stem cells in the fetal brain are the predominant cell type affected during development by CMV. Cheeran et al21 proposed possible mechanisms of CMV developmental disruption, including direct damage followed by reduction in the number of neural stem cells or intermediate progenitors; alterations in stem cell migration and fate of cell differentiation; infection of astroglia, causing disruption of their normal supportive functions; and alterations in the microenvironment of the developing brain due to cytokines and soluble factors generated by resident glial cells.

These combined factors may produce not only malformative pathologies of different severity, including microcephaly and malformations of cortical development22 (Figure 9–2), but also direct injury to the brain, resulting in ventriculomegaly, calcifications, brain atrophy, cyst formation, or hemorrhage.22,23
Figure 9–2.
Polymicrogyria in a fetus at 31 postmenstrual weeks with CMV infection. Low field magnification. Note the transition from an almost normal six-layer cortex to the zone with polymicrogyria. Similar foci of polymicrogyria were found in other locations. (Courtesy of Dr. Letizia Schreiber, Holon, Israel.)

Fetal CMV infection may affect other systems and organs. Reported gastrointestinal findings include hyperechogenic intestines,24,25,26 bowel dilation,27 hepatomegaly and/or splenomegaly,24,26,28,29 and liver calcifications.25 In our experience, a frequent early sign of infection is hyperechogenic intestines. It is rarely observed as an isolated finding, and it is usually transient.
Rarely, fetal CMV infection may involve the heart and cause cardiomegaly,29 endocardial fibroelastosis with hypoplastic left heart,29 and cardiomyopathy.24 Growth restriction, hydrops, and oligohydramnios are frequently present;24,25,26,29 however, hydrops and oligohydramnios may be transient and resolve following the acute stages of the fetal disease. Placental thickness is significantly increased in infected fetuses.29,30
When a diagnosis is reached during pregnancy, multiple organ involvement may be present in as much as 42% of the patients.29
Although uncommon recurrent maternal CMV infection may produce fetal disease, this may be due to reactivation of the disease or more probably to infection by a different strain.20 It is usually recognized that in these fetuses the infection may be mild or even subclinical, but according to our personal experience and also to isolated cases reports, this assumption may not necessarily be true.31,32,33,34 During a 3-year period, Zalel et al34 found six fetuses with sonographic findings characteristic of CMV infection whose mothers were known to be CMV seropositive before or at the beginning of the index pregnancy; five out of six fetuses had severe brain involvement.
Well-documented cases of the consecutive occurrence of fetal CMV infection in the same woman are extremely rare. Stagno et al35 described in 1973 two pregnant women who delivered affected siblings. The interval between the pregnancies was 17 and 14 months, respectively, and in both cases, the younger children were asymptomatic.
It is important to remember that, in these cases, the differential diagnosis includes the possibility of fetal disease due to a different infective agent and the autosomal recessive Aicardi-Goutières (pseudo-TORCH [toxoplasmosis, other infections, rubella, cytomegalovirus, and herpes simplex virus) syndrome.36
Fetal CNS signs of congenital CMV infection were first described in the 1980s37 and are similar to those reported in newborns.38 Although ventriculomegaly of different grades of severity, calcifications, and microcephaly are the more frequent presenting signs, abnormal periventricular echogenicity with or without cysts is consistently present in severely affected fetuses.
CMV may produce a very wide spectrum of brain pathologies according to the period of brain development in which the infection starts and probably also to the virulence of the virus or the immunological status of the mother and fetus. The general understanding is that early infection produces a more severe and generalized pattern of disease, whereas late infection produces a milder disease.39
Increased periventricular echogenicity is best depicted by transvaginal sonography (Figures 9–3 and 9–4). Characteristically, it involves the whole periventricular zone of both hemispheres, and it is well demarcated from the remaining brain parenchyma. Cysts and calcifications may be found within the zones of increased echogenicity. Cyst formation may be the result of parenchymal necrosis or liquefaction of small zones of hemorrhage; we have observed that in some cases the cyst walls, when adjacent, undergo lysis, and a larger porencephalic cyst is formed40 (Figure 9–5). The presence of abnormal periventricular findings may be depicted in some, but not all, patients during a routine transabdominal examination using axial planes (Figure 9–6).
Figure 9–3.
Transvaginal parasagittal planes. (A) Normal fetus at 24 postmenstrual weeks. The echogenicity of the brain parenchyma is similar throughout the whole surface. (B–F) Five fetuses with proven CMV at different gestational ages showing a clearly demarcated hyperechogenic periventricular zone (arrows). Not all of the affected fetuses have ventriculomegaly. Note the presence of punctuate calcifications (B, F), periventricular cysts (D, E), and intraventricular adhesions (E, F).

Figure 9–4.
Transvaginal coronal planes. (A) Normal transthalamic section at 25 postmenstrual weeks. The thalami are slightly more echogenic than the brain. (B–F) Increased periventricular echogenicity with clear demarcation from the remainder of the brain (arrows) in five fetuses with CMV at different gestational weeks. Transfrontal plane (D), transcaudate plane (B, F), transthalamic plane (C), and transoccipital plane (E). Coarse calcifications and abnormal sulcation with early development of numerous shallow sulci are present in the fetus at 29 weeks of gestation (F).

Figure 9–5.
Transvaginal parasagittal planes. Periventricular occipital cysts (A) at 24.5 postmenstrual weeks converting into a larger porencephalic occipital cyst or intraventricular adhesion (B) 2 weeks later. (From Malinger G, Lerman-Sagie T. Fetal cytomegalovirus infection: The brain as a window in the establishment of prognosis. In: Ramenghi A, Evrard P, Mercuri E, eds. Mariani Foundation Paediatric Neurology. Perinatal brain damage: From Pathogenesis to Neuroprotection. Vol 19. Montrouge: Editions John Libbey Eurotext; 2008;49–54, with permission.)

Figure 9–6.
Transabdominal axial planes at the level of the lateral ventricles. (A–B) Images of fetuses with known CMV infection and periventricular hyperechogenicity show that it is clearly differentiated from the surrounding brain (arrows). Both fetuses (A) at 24 weeks, (B) at 26 weeks, presented with porencephalic occipital cysts (arrowheads) but without ventriculomegaly.

Intracranial calcifications involving the brain parenchyma, thalami, basal ganglia, and cerebellum can be demonstrated in at least some cases, starting from the second trimester. The calcifications may be punctuate or coarse; regional, isolated, diffuse, or in clusters (see Figures 9–3 and 9–4). Coarse echogenicities adjacent to the lateral ventricles may represent an end stage of periventriculitis. The differential diagnosis of intracranial calcifications includes other infectious agents, intracranial teratomas, tuberous sclerosis, Sturge-Weber syndrome, Aicardi-Goutières syndrome, and sagittal or transverse sinus thrombosis.36,41,42,43,44,45,46
Microcephaly is consistently observed but may not be obvious during the second trimester or even the early third trimester; in many cases, microcephaly is accompanied by brain atrophy (Figure 9–7). Migration and organization disorders ranging from focal sulcal anomalies to generalized lesions40,47 (see Figures 9–4 and 9–7) are usually found in fetuses with severe involvement.
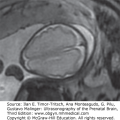
Figure 9–7.
Orthogonal views of a fetus with CMV at 24 weeks, 2 days; the head circumference (HC) was 20 cm (<–2 SDs [standard deviations]). Axial (A), coronal (B), and sagittal (C) views. Note the enlarged subarachnoidal space (1), the underdeveloped sylvian fissure (2), and the presence of an abnormal sulcus in the frontal lobe (3). The small coronal figure provides an image for comparison of a normal fetus at 22 weeks of pregnancy.

Congenital CMV may affect the white matter; this pattern of disease has been described in children and adults48 but may also be depicted during fetal life, usually late in the third trimester (Figure 9–8). Callosal dysgenesis may be the result of this type of insult.22,40
Figure 9–8.
CMV in a fetus at 35 postmenstrual weeks; (A) axial, (B) coronal, (C) sagittal. The mother was CMV seropositive during the first trimester and was referred because of ventriculomegaly (1) at a routine ultrasound (US) examination. Bilateral large intraventricular cysts (2) and small periventricular pseudocysts (3) are depicted. The sulci and gyri are not observed due to white matter involvement (4).

Estroff and colleagues49 reported the presence of branching linear echogenic areas in the thalami of a fetus with CMV. This entity is frequent in the neonatal period and was initially considered a characteristic sign of infection.50,51 The current approach is that it represents a nonspecific sign, as it has also been described in children with asphyxia, chromosomal anomalies, metabolic diseases, maternal heroin abuse, and in the recipient in twin-to-twin transfusion syndome.38 Single or ramified linear echo densities, produced by hyalinization or mineralization of the perforating striatal arteries, are better visualized in the parasagittal plane (Figure 9–9). Striatal arteries originate from the middle cerebral arteries and irrigate the germinal matrix and when normal are not depicted.

Although extremely uncommon, isolated cases of cerebral52,53 and cerebellar54 hemorrhages have been reported. The cerebellum may also be involved demonstrating calcifications, cysts,22,40 or a reduction in size.
Two recent retrospective studies have compared fetal ultrasound (US) and magnetic resonance imaging (MRI) findings in patients with CMV. Picone and colleagues55 studied 38 fetuses in which CMV polymerase chain reaction (PCR) was positive in the amniotic fluid.55 MRI failed to show any sign of brain infection in 11 fetuses with normal US examinations. In 13 fetuses in which US only depicted extracerebral findings, MRI detected brain lesions in 46%. MRI confirmed the presence of cerebral signs found by US in the remaining 14 fetuses and in some of them added new information that was not depicted by US.55 Benoist and colleagues23 studied by targeted US and MRI 49 fetuses with proven CMV infection and compared the results to the postnatal US or post mortem examinations; the best positive predictive value (88.9%) was obtained when both US and MRI showed abnormal findings, and the best negative predictive value (93.5%) was obtained when the US was normal.
We have seen five CMV PCR-positive fetuses in whom there was a discrepancy between the US and MRI findings. The US was normal, whereas the MRI raised the suspicion of white matter abnormalities. Three children were delivered and were developing normally at ages 2 to 4 years; two pregnancies were terminated, and the autopsies were negative for brain CMV; but in one patient microglial nodules consistent with an inflammatory reaction were found. Garel56 reported that in all patients with a normal US the MRI was also normal.
Neurosonography and MRI perform equally in the demonstration of morphological anomalies (Figures 9–10 and 9–11).

Figure 9–11.
Sagittal transvaginal US and magnetic resonance imaging (MRI) at 29 postmenstrual weeks in a fetus with CMV. The MRI examination was performed 3 days after the US. Parasagittal US (A) and MRI (B) show mild ventriculomegaly with irregular, dentate ventricular walls (arrows) due to ventriculitis and ependymal damage. More lateral US (C) and MRI (D) views show a wide sylvian fissure and almost complete lack of sulcation.

Due to the low prevalence of symptomatic congenital CMV infection, the low sensitivity and specificity of the available tests, and the lack of proven intrauterine treatments, universal screening for CMV infection is not an integral part of prenatal care. In these patients, second- or third-trimester US examinations are the only opportunity to raise the suspicion of fetal disease. The presence of any of the extracerebral findings described previously should prompt the performance of serological tests and a detailed brain examination for CMV signs. Before 20 weeks, the only described sign of fetal infection is intestinal hyperechogenicity; later on the presence of hepatosplenomegaly, ascites, or cardiomegaly should be considered suspicious. During routine second-trimester examinations, the presence of ventriculomegaly or intracranial calcifications is a clear indication for further investigation. In these patients, a careful analysis of the periventricular zone is of paramount importance, as in the vast majority of patients with CMV, this region will be involved.22,40
The earliest reports of US recognition of CMV-related findings are at 19–20 weeks.27,53 In our series, the earliest diagnosis was suspected at 20 weeks in a fetus with echogenic bowel, increased periventricular echogenicity, and abnormal sulcation (Figure 9–12).
Figure 9–12.
Early detection of CMV infection in a fetus at 20 postmenstrual weeks. (A) Transabdominal image showing hyperechogenic intestines (arrow). (B) Sagittal plane. Note the well demarcated periventricular echogenicity (arrow) with increased amount of subarachnoid fluid due to reduced cerebral size (arrowhead). (C) Axial plane at the level of the lateral ventricle. Hyperechogenic cerebral surface is consistent with early abnormal sulcation and probable polymicrogyria (arrows).

Targeted US examinations are of paramount importance in the management of fetuses with proven intrauterine infection and of those in whom maternal seroconversion has occurred during pregnancy, but the fetal status is unknown. Although not conclusively proven, most authorities believe that the presence of microcephaly or intracranial findings is associated with a poor prognosis, and in these cases termination of pregnancy or experimental antiviral treatments may be considered.20,57
Affected fetuses with normal targeted US examinations should be followed with repeated targeted examinations at 3- to 4-week intervals.
Prognosis is based on the extent of involvement, particularly of the brain. If the examination remains normal, the prognosis appears to be excellent.40 It is important to remember that a normal US examination will never be able to rule out sensorineural hearing loss (SNHL).
Although not always feasible, accurate knowledge of the gestational week in which the fetus was infected is an important parameter in counseling.58 Maternal seroconversion during the third trimester implies fetal infection, as CMV is highly transmissible but is almost invariably asymptomatic.59
Recently, Foulon and colleagues60 described the follow-up of 28 delivered children who had proven intrauterine fetal infection; 4 out of 5 children with first-trimester infection had SNHL, but all 12 children with third-trimester infection were unaffected.
Because most of the infected newborns are asymptomatic and thus not diagnosed, it is difficult to predict the risks of an abnormal neurodevelopmental outcome and/or SNHL in the whole affected population. Based on longitudinal studies, 85% to 100% of patients with asymptomatic disease will develop normally,48,61,62,63 and only 1 out of 100 children will develop SNHL per year of follow-up.64 The prognosis of affected fetuses with abnormal neurosonography during pregnancy can be predicted by extrapolating from existing data regarding the bad prognosis in newborns with symptomatic CMV and brain computed tomography or US signs of infection.57,65 The prognosis remains unclear in patients with positive detection of CMV in the amniotic fluid who present with either isolated minor brain findings, such as periventricular pseudocysts or striatal vasculopathy, or isolated systemic findings.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


