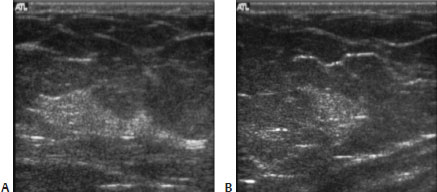
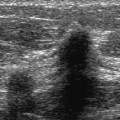
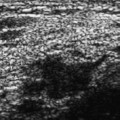
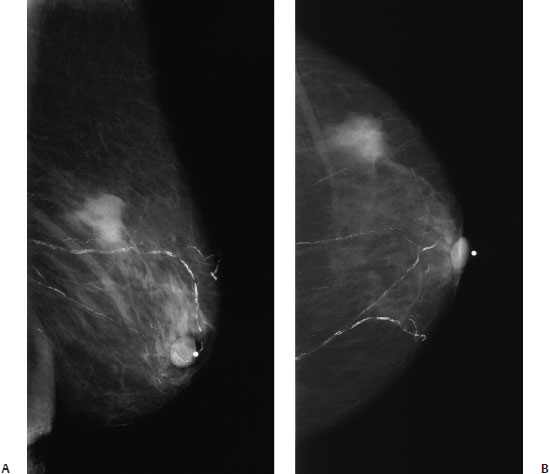
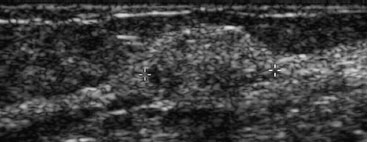
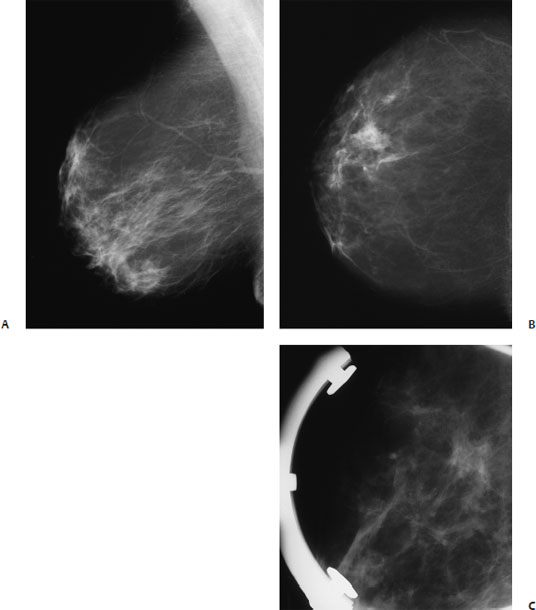
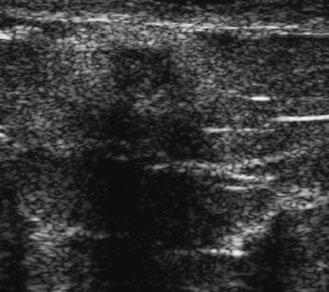
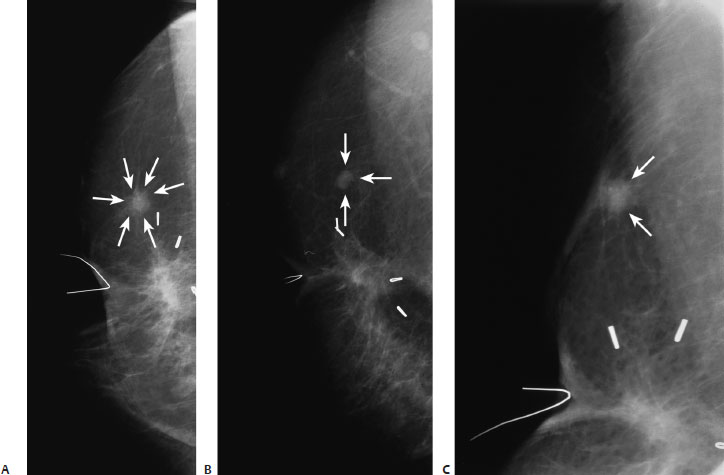
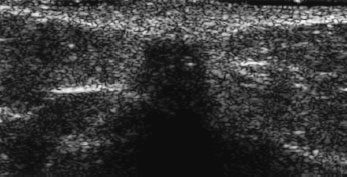
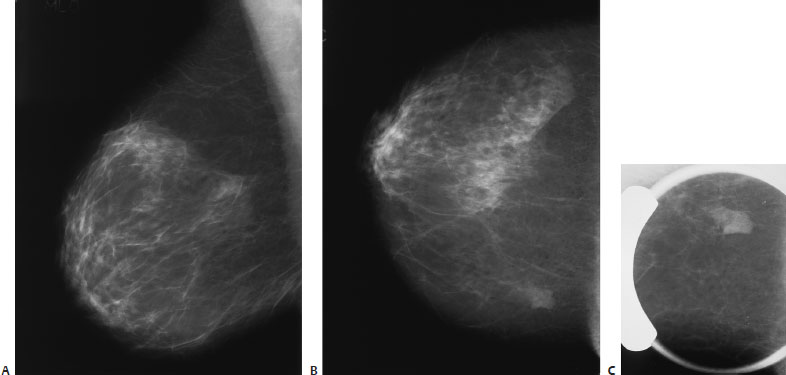
7 Irregular Masses: Benign Masses An 86-year-old woman presents with a new left breast palpable lump. • Left breast: palpable lump in upper outer quadrant • Right breast: normal exam Mass (Fig. 7.1) • Margin: indistinct • Shape: irregular • Density: equal density Fig. 7.1 In the left upper outer quadrant, there is an irregular mass that corresponds to the palpable lump. (A) Left MLO mammogram. (B) Left CC mammogram. Frequency • 8 MHz Mass (Fig. 7.2) • Margin: ill defined • Echogenicity: hyperechoic • Retrotumoral acoustic appearance: posterior shadowing distal to mass • Shape: ellipsoid Fig. 7.2 Left radial breast sonogram. The palpable mammographic mass corresponds to a hyperechoic oval mass, which has a partially ill-defined margin. • Microglandular adenosis • BI-RADS assessment category 4, suspicious; biopsy should be considered. • Microglandular adenosis is a rare type of adenosis. Most patients present with a palpable lump. • There are no specific radiographic or sonographic patterns for this disease due to its rarity. • Microglandular adenosis has been associated with infiltrating carcinoma, so lesions that increase in size should be critically reevaluated. James BA, Cranor ML, Rosen PP. Carcinoma of the breast arising in microglandular adenosis. Am J Clin Pathol 1993;100:507–513 Rosen PP. Microglandular adenosis. A benign lesion simulating invasive mammary carcinoma. Am J Surg Pathol 1983;7:137–144 Rosenblum MK, Purrazzella R, Rosen PP. Is microglandular adenosis a precancerous disease? A study of carcinoma arising therein. Am J Surg Pathol 1986;10:237–245 Tavassoli FA. Benign lesions. In: Tavasolli FA, Fattaneh A, eds. Pathology of the Breast. 2nd ed. Stamford: Appleton and Lange; 1999:115–204 A 60-year-old woman presents with a new right breast lump. She has no previous trauma, breast surgery, or biopsy. • Right breast: palpable lump at the 11 o’clock position • Left breast: normal exam Mass (Fig. 7.3) • Margin: indistinct • Shape: irregular • Density: equal density Fig. 7.3 In the right upper outer quadrant, there is an irregular mass that corresponds to the palpable mass. (A) Right MLO mammogram. (B) Right CC mammogram. (C) Right MLO spot compression mammogram. Frequency • 11.5 MHz Mass (Fig. 7.4) • Margin: ill defined • Echogenicity: heterogeneous • Retrotumoral acoustic appearance: posterior shadowing distal to mass • Shape: irregular Fig. 7.4 Right radial breast sonogram. The palpable mammographic mass corresponds to an ill-defined irregular mass with a hyperechoic rim and hypoechoic center. The mass exhibits severe acoustic shadowing. • Fat necrosis • BI-RADS assessment category 4, suspicious; biopsy should be considered. • Although only 40% of patients with fat necrosis have a history of previous breast injury, this lesion has a traumatic origin. Fat necrosis has two different appearances. In some patients, the fat necrosis causes a fibrotic response that results in an irregular solid mass (illustrated in this case), which may be associated with skin thickening and nipple retraction. This mass cannot be distinguished mammographically or sonographically from carcinoma. Besides producing an irregular mass, fat necrosis may also produce a lipid collection without an inflammatory response. This second type of fat necrosis results in a round or oval nodule (oil cyst) that is either calcium or fat density mammographically. Bassett LW, Gold RH, Cove HC. Mammographic spectrum of traumatic fat necrosis: the fallibility of “pathognomonic” signs of carcinoma. AJR Am J Roentgenol 1978;130:119–122 Evers K, Troupin RH. Lipid cyst: classic and atypical appearances. AJR Am J Roentgenol 1991;157:271–273 Orson LW, Cigtay OS. Fat necrosis of the breast: characteristic xeromammographic appearance. Radiology 1983;146:35–38 A 72-year-old woman status-post right lumpectomy and radiation therapy has developed a new mammographic finding near the surgical site. This is the same patient as Case 7.9. • Right breast: subareolar scar • Left breast: normal exam Mass (Fig. 7.5) • Margin: spiculated • Shape: irregular • Density: equal density Fig. 7.5 There is a spiculated density deep to the right nipple. This density corresponds to the scar from the patient’s lumpectomy. In the upper outer breast, there is a spiculated mass (arrows), which is separate from the main scar. This spiculated mass is new since the patient’s previous exam. (A) Right LM mammogram. (B) Right CC mammo-gram. (C) Right mammogram tangential to spiculated mass (arrows). Frequency • 10 MHz Mass (Fig. 7.6) • Margin: ill defined • Echogenicity: hypoechoic • Retrotumoral acoustic appearance: severe shadowing • Shape: irregular Fig. 7.6 Right radial breast sonogram. In the upper outer quadrant, the new small spiculated mammographic mass corresponds to an ill-defined hypoechoic shadowing mass. The hyper-echoic halo around the mass corresponds to the mammographic spiculations. • Fat necrosis: the new spiculated mass in the right upper outer quadrant corresponded to fat necrosis. • BI-RADS assessment category 4, suspicious; biopsy should be considered. • When fat necrosis causes new irregular masses in the area of a lumpectomy site, this abnormality cannot be distinguished from malignancy mammographically or sonographically. Sohn C, Blohmer J-U, Hamper UM. Sonography in the follow-up of breast cancer. In: Sohn C, Blohmer J-U, Hamper UM, eds. Breast Ultrasound. New York: Thieme; 1999:98–102 Tohno E, Cosgrove DO, Sloane JP. Postoperative scarring. In: Tohno D, Cosgrove DO, Sloane JP, eds. Ultrasound Diagnosis of Breast Diseases. New York: Churchill Livingstone; 1994:146–147 A 49-year-old woman presents with a new density on her right screening mammogram. • Normal exam Mass (Fig. 7.7) • Margin: indistinct • Shape: irregular • Density: equal density Fig. 7.7 In the right upper medial breast, there is an irregular mass that is partially obscured by the dense overlapping breast tissue. (A) Right MLO mammogram. (B) Right CC mammogram. (C) Right CC spot compression mammogram. Frequency • 7.5 MHz Mass (Fig. 7.8) • Margin: ill defined • Echogenicity: hyperechoic • Retrotumoral acoustic appearance: posterior shadowing distal to mass • Shape: irregular Fig. 7.8 Right breast sonogram. The irregular density identified in Fig. 7.7 corresponds to a homogeneously hyperechoic irregular mass. (A) Right radial breast sonogram. (B) Right radial breast sonogram. A B • Fibroadenoma • BI-RADS assessment category 4, suspicious; biopsy should be considered. • Fibroadenomas are the most common mass in women younger than 40 years of age. Researchers have reported that these masses are present in 9 to 25% of autopsy cases. The highest incidence of fibroadenomas is in women younger than 25 years of age.
Case 7.1: Adenosis
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 7.2: Fat Necrosis
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 7.3: Fat Necrosis
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 7.4: Fibroadenoma
Case History
Physical Examination
Mammogram
Ultrasound
Pathology
Management
Pearls and Pitfalls
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine