Knee Dislocation
Adam T. Ryan
Daniel B. Nissman
CLINICAL HISTORY
Motor vehicle crash.
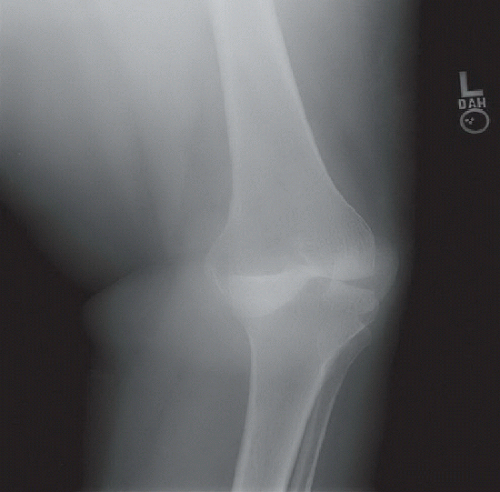 FIGURE 82A |
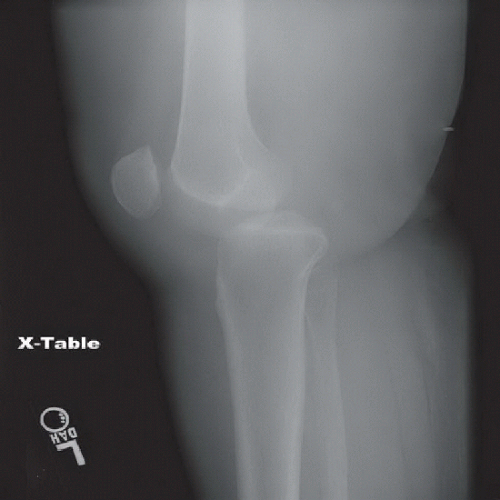 FIGURE 82B |
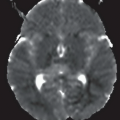
 FIGURE 82C |
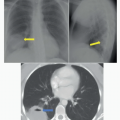
 FIGURE 82D |
FINDINGS
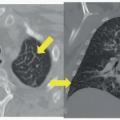
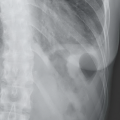
Supine AP (Fig. 82A) and cross-table lateral (Fig. 82B) radiographs of the left knee demonstrate posterior and slight lateral displacement of the tibia relative to the femur with marked varus angulation. The patella is also displaced laterally. No fracture is seen. Sagittal MR image (Fig. 82C) demonstrates marked posterior displacement of the tibial plateau and completely torn anterior (short arrow) and posterior cruciate ligaments (long arrow); the femoral attachment of the fibular collateral ligament was also avulsed (not shown). Oblique sagittal reformatted image from a CT
angiogram (Fig. 82D) of the popliteal fossa demonstrates an opacified popliteal artery to the level of the tibiofemoral joint beyond which it is unopacified, consistent with complete occlusion.
angiogram (Fig. 82D) of the popliteal fossa demonstrates an opacified popliteal artery to the level of the tibiofemoral joint beyond which it is unopacified, consistent with complete occlusion.
DIFFERENTIAL DIAGNOSIS
Anterior, posterior, medial, lateral, or rotary knee dislocation with/without associated neurovascular injury.
DIAGNOSIS
Posterior knee dislocation with associated ligamentous and popliteal artery injuries.
DISCUSSION
Knee dislocations are rare, usually resulting from extreme trauma, and can be limb-threatening from associated neurovascular damage. The true frequency of knee dislocations is unknown because of the possibility of reduction, spontaneous or otherwise, prior to evaluation by a physician or because of other distracting injuries in the polytrauma setting. Unreduced dislocations usually present with obvious physical examination findings, but spontaneously reduced dislocations can lead to underestimation of the severity of injury, thereby risking the limb.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


