Chapter 2
Liver Mass
• Describe the sonographic appearance of commonly encountered benign liver neoplasms.
• Describe the sonographic appearance of commonly encountered malignant liver neoplasms.
• Differentiate the Doppler findings in various liver neoplasms.
• List the risk factors associated with specific lesions of the liver.
• Identify pertinent laboratory values associated with specific liver neoplasms.
CLINICAL SCENARIO
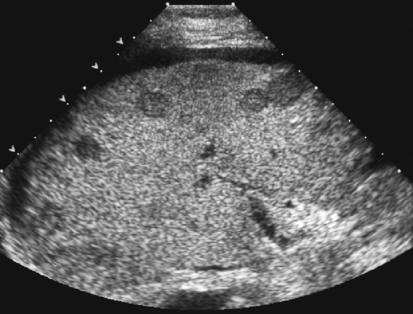
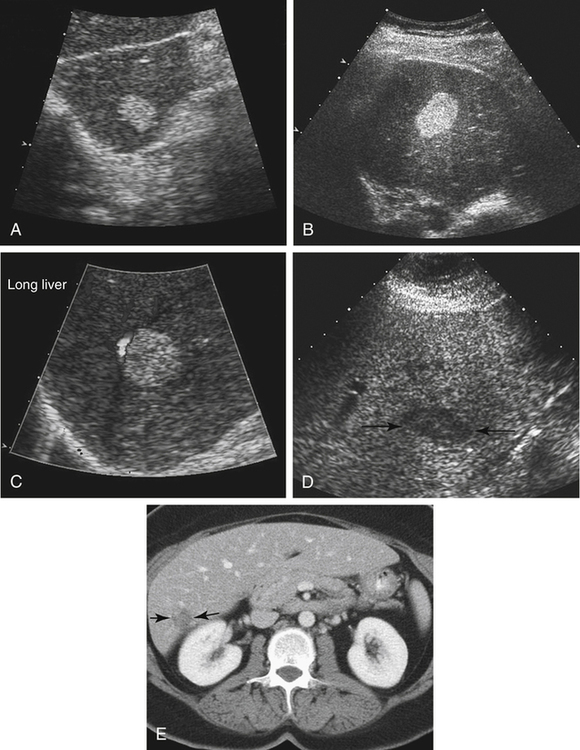
An 84-year-old woman is seen in the sonography department for a diagnostic paracentesis and biopsy of hepatic masses seen on computed tomography (CT). She has a past history of total hysterectomy and unilateral salpingo-oophorectomy (25 years ago). She was recently found to have a large pelvic mass and markedly elevated cancer antigen 125 (CA 125) level. Multiple small hepatic masses are seen (Fig. 2-1). A core biopsy sample is taken from one of the masses and sent to the pathology laboratory. What is the pathology report most likely to reveal?
Liver
Normal Sonographic Anatomy
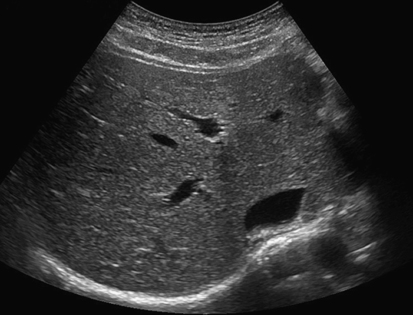
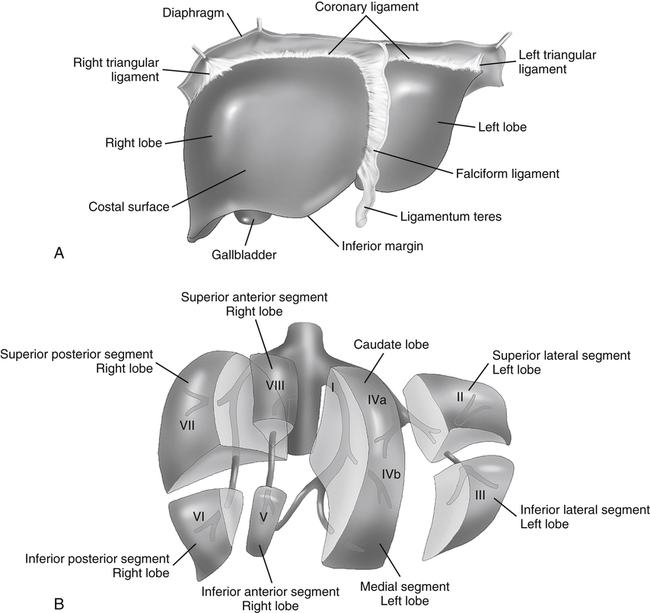
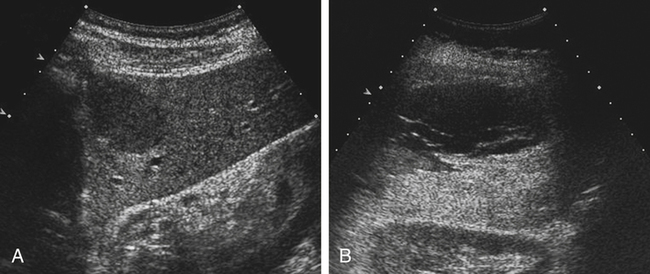
The liver is located in the right upper quadrant and extends partially into the left upper quadrant. Normal liver parenchyma should appear homogeneous and display midlevel echogenicity (Fig. 2-2). Compared with the renal parenchyma, normal liver parenchyma appears slightly hyperechoic or isoechoic, and compared with the pancreas, the liver appears slightly hypoechoic or isoechoic. Within the parenchyma, tubular structures corresponding to veins, arteries, and ducts can also be visualized. The average size of the liver is less than 15 cm in length at the midclavicular line, but size varies with patient height and weight. The liver is divided into three lobes: right, left, and caudate (Fig. 2-3, A). The right lobe is divided into anterior and posterior segments; the left lobe is divided into lateral and medial segments. Couinaud’s classification more precisely divides the liver into eight segments (Fig. 2-3, B). Accurate documentation of the location of a mass is important for follow-up imaging, surgical excision, and treatment.
Benign Masses
Hepatic Cyst
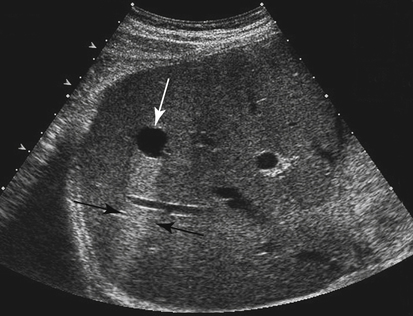
True cysts of the liver are found with sonography in 2.5% to 10% of the general population.1 Their exact origin is unclear, although it is thought to be ductal. Generally, hepatic cysts are discovered incidentally. Patients are asymptomatic unless the cyst becomes infected or hemorrhages. The incidence of hepatic cysts increases with age. The likelihood that they are clinically relevant is low.
Hemangioma
Cavernous hemangiomas are the most common benign tumors of the liver. Cavernous, blood-filled channels make up these lesions. Hemangiomas are found with sonography in 0.7% to 1.5% of the population, although the incidence at autopsy reaches 20%.1 Most hemangiomas are small and asymptomatic and are discovered incidentally. They are typically found in adults, and are more common in women than men. Although patients are usually asymptomatic, larger hemangiomas may cause pain because of hemorrhage or rupture.
Sonographic Findings
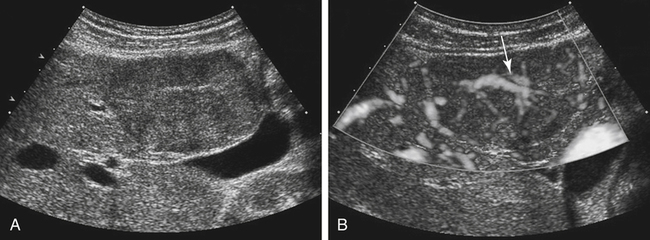
The most common appearance of a cavernous hemangioma is a well-defined, hyperechoic mass that may be round, oval, or lobulated. Acoustic enhancement may be seen because of the vascular nature of this lesion. The sonographic appearance of hemangiomas may also be of variable echogenicity depending on the size of the lesion and the amount of fibrosis and degeneration. Because of the low flow of blood within a cavernous hemangioma, color Doppler and power Doppler are of little use in the characterization of hemangiomas (Fig. 2-5).
Focal Nodular Hyperplasia
Focal nodular hyperplasia (FNH) is the second most common benign liver mass after hemangioma. FNH is believed to be a hyperplastic area of normal liver cells that is associated with a congenital vascular malformation. A distinguishing feature of FNH is that it has a central stellate scar. Incidence of the scar at autopsy ranges from 0.3% to 3%.1 Female hormones are believed to play a role in the development of FNH because it is most often seen in women of childbearing age. It is usually asymptomatic and discovered incidentally, as a solitary lesion in the right lobe.
Sonographic Findings
Because FNH is comprised of liver cells, it is often isoechoic to the liver parenchyma and can be very subtle. A change in the contour of the liver or displacement of vascular structures is often a clue to its existence. FNH may also appear hypoechoic or hyperechoic. Color Doppler or power Doppler is useful in identification of the prominent vascularity of the central stellate scar (Fig. 2-6).
Hepatocellular Adenoma
Hepatocellular adenoma may be silent, or it may be discovered as a mass on physical examination. The patient may present with pain if the mass has hemorrhaged. Because the incidence of hepatocellular adenoma is greater in women taking oral contraceptives than in women who are not, these masses have been seen to regress with cessation of oral contraceptive therapy and to increase in size during pregnancy.1 Because of the tendency for hepatocellular adenoma to develop into serious complications, surgical resection is the recommended treatment.
Sonographic Findings
The sonographic appearance for hepatocellular adenoma is varied and nonspecific. Fat content may cause it to be hyperechoic, or it may be hypoechoic. Hemorrhage within the lesion may appear anechoic, hypoechoic, or hyperechoic (Fig. 2-7). Color Doppler imaging may show the significant peripheral vasculature of this lesion.2






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


