and Robert W. Henderson3
(1)
Kaiser Permanente, Southern California Permanente Medical Group, Riverside, CA, USA
(2)
Molecular Imaging Center and PET Clinic, University of Southern California, Los Angeles, CA, USA
(3)
Department of Radiology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
Case 9.1: Transformation of Follicular Lymphoma Grade
History
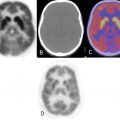
A 63-year-old female with recurrent lymphoma. Patient had low-grade (grade 1A) follicular B-cell lymphoma initially in the left inguinal region. The current disease is follicular B cell (grade 3). Scan is requested for restaging.
Findings
There are at least two subcentimeter left cervical level 2 lymph nodes with the most active with maximum SUV of 8.6 (Fig. 9.1). There is a subcentimeter left level 5 lymph node with maximum SUV of 7.9. These are consistent with lymphomatous involvement. There are multiple splenic lesions noted with the largest and most active measuring 2.4 cm × 1.8 cm, with maximum SUV of 13.9 correlating to hypodense region on CT.

Fig. 9.1
Pearls and Pitfalls
Recurrent disease with histopathological transformation from grade 1–3 (Fig. 9.1).
Case 9.2: Multiple Recurrences with High-Grade Transformation of Lymphoma
History
A patient with low-grade follicular lymphoma initially diagnosed in the sacrum in 1998, treated with chemotherapy and radiation. A patient had recurrence in 2004 involving the right groin, bilateral iliac region, and right base of the tongue, treated with chemotherapy and radiation therapy. No interval treatment since then. Current study in 2011.
Findings
Interval increase in size and metabolic activity of a left level 4 node now measuring 1.2 cm in short axis with SUVmax 4.5 (normal size and inactive in prior) (Fig. 9.2). New intensely active and enlarged left porta hepatis nodes, SUVmax up to 12. There is interval increase in metabolic activity but unchanged size of a left retroaortic node, now with SUVmax 4.3 (SUVmax 3.8 in prior).

Fig. 9.2
Pearls and Pitfalls
1.
Multiple recurrences with progressive more biologic activity as noted with SUVmax in the current study.
2.
Zevalin (90Yt Rituxan) with higher response rate than Rituxan alone.
Discussion
Follicular lymphoma is the second most common type of lymphoma in high-income countries, representing nearly 20 % of all non-Hodgkin’s lymphomas. The pathogenesis of follicular lymphoma remains elusive, and evidence exists that t(14;18)(q32;q21), the most common genetic alteration in follicular lymphoma cells, which results in an overproduction of the antiapoptotic BCL-2 protein, is not sufficient to cause the disease [26]. By contrast, the role of infiltrating cells in the tumor microenvironment has gained attention in the past few years [1]. The clinical course of follicular lymphoma is quite variable, with some patients having an indolent, waxing, and waning disease for years, without the need for therapy, and others presenting with a more disseminated and rapidly growing disease. Most patients with follicular lymphoma have incurable disease, with a generally indolent course, frequent relapses, and a progressive decrease in duration of responses with every subsequent relapse. A major advance in the treatment of follicular lymphoma was the introduction of monoclonal antibodies to therapeutic regimens, mainly antibodies against CD20. These antibodies have contributed to the improvements in survival of patients with follicular lymphoma recorded in the past decade [2]. But, even in the immunotherapy era, relapses will occur (Fig. 9.2).
Case 9.3: Diffuse Large B-Cell Lymphoma Scapula
History
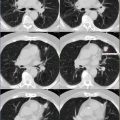
A patient with diffuse large B-cell lymphoma, stage 4, involving the right scapula (biopsy dated 12/13/2010). No treatment yet.
Findings
A hypermetabolic, osteolytic right scapular body mass involving the wing and extending into the glenoid, with SUVmax 10.3 consistent with biopsy-proven lymphoma (Fig. 9.3). Hypermetabolic, right supraclavicular and right axillary nodes (faintly visible) with SUVmax up to 6.5 and hypermetabolic right inguinal node (1.3 cm, with SUVmax 13.2) are consistent with lymphomatous involvement (Fig. 9.3).

Fig. 9.3
Case 9.4: Hodgkin’s Lymphoma Involving Spine
History
A 47-year-old female presenting with neurologic symptoms, undergoing workup with PET-CT for T5 lesion, status post bone biopsy which was nondiagnostic. However, post scan biopsy reported classic Hodgkin’s lymphoma.
Findings
There is a large hypermetabolic mass involving T5 with its soft tissue component causing bony destruction and extending posteriorly abutting and possibly causing mass effect on the spinal cord, SUVmax 13.3 (Fig. 9.4). This lesion extends anteriorly to abut the posterior aspect of the trachea and extends laterally involving adjacent paravertebral space (Fig. 9.4).

Fig. 9.4
Case 9.5: Sacral Lymphoma
History
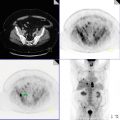
A 59-year-old male with B-cell lymphoma of the right sacrum.
Findings
Intensely active destructive lytic mass involving the right sacral wing and body with presacral extension of the soft tissue, with maximum SUV of 12.5 (Fig. 9.5). In addition, there is extension of this lesion into the adjacent iliacus musculature. There is extension into the lower bony spinal canal with involvement of the first and second sacral foramina (Fig. 9.5).

Fig. 9.5
Case 9.6: Right Maxillary Lymphoma
History
A 71-year-old male with history of diffuse large B-cell lymphoma involving the right maxilla and right neck nodes for initial staging.
Findings
There is a large right maxillary sinus mass with SUVmax 15 (Fig. 9.6). There is osseous destruction involving the anterior and medial walls of the right maxillary sinus as well as the maxilla.

Fig. 9.6
Discussion
Primary lymphoma of the bone is a rare malignant condition that accounts for less than 5 % of all primary bone tumors [3]. It has also been called reticulum cell sarcoma [4], malignant lymphoma of the bone [5], and more recently osteolymphoma [6]. The vast majority of cases are of the non-Hodgkin type, with Hodgkin’s disease accounting for 6 % of cases in one series [3]. Lymphomas of the bone are uncommon, comprising only 8 % of primary malignant bone tumors [3]. Most malignant lymphomas of the bone are diffuse non-Hodgkin’s lymphomas of B-cell type [4] (Fig. 9.6).
Case 9.7: NHL Bladder
History
Primary urinary bladder non-Hodgkin’s lymphoma in an 80-year-old female. She presented with difficulty urinating and urinary frequency and urgency along with weak stream of urine. On physical examination, she was found to have bladder neck mass for which she underwent transurethral resection of the mass. The pathology was consistent with diffuse large B-cell lymphoma.
Findings
Staging PET-CT study demonstrated a hypermetabolic, soft tissue mass at the base of the urinary bladder, measuring 6.3 × 3.8 × 3.4 cm and maximum SUV of 21.8 (Fig. 9.7). She had received chemotherapy and demonstrated excellent response on the follow-up PET-CT study.

Fig. 9.7
Pearls and Pitfalls
Lymphomas of the bladder are rare lesions, representing approximately 0.2 % of the primary neoplastic lesions and approximately 1.8 % of the secondary lesions in this organ [7, 8, 27].
Discussion
Primary lymphoma of the bladder represents 0.2 % of all bladder malignancies. Secondary involvement of the bladder by malignant lymphoma occurs in 10–50 % of cases. Most lymphomas of the bladder are non-Hodgkin’s lymphomas of the B-cell type, with preponderance among women. Patients with bladder lymphomas can be divided into three groups, according to their clinical presentation: (1) primary cases in the bladder, (2) cases occurring in the bladder as a manifestation of systemic disease, and (3) secondary cases, with clinical history of malignant lymphoma recurring in the bladder. In the latter case, the main sites of involvement are peripheral lymph nodes, the bone marrow, and the spleen [8] (Fig. 9.7).
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


