CHAPTER 17 Magnetic Resonance Evaluation of Blood Flow
DESCRIPTION OF TECHNICAL REQUIREMENTS
Phase Contrast Magnetic Resonance Imaging
Velocity-encoded cine phase contrast MRI employs a bipolar gradient pulse to encode the velocity of moving protons. The two lobes of the bipolar gradient pulse are equal in strength but opposite in orientation, one positive, the other negative. A stationary proton will experience equal and opposite gradients that cancel one another and will have no resulting phase shift. However, a moving proton will not experience an equal but opposite second lobe of the gradient pulse and consequently will acquire a phase shift (Fig. 17-1). The angle of acquired phase shift is proportional to the velocity of the moving proton. An MRI sequence with this type of bipolar gradient is thus flow sensitive.
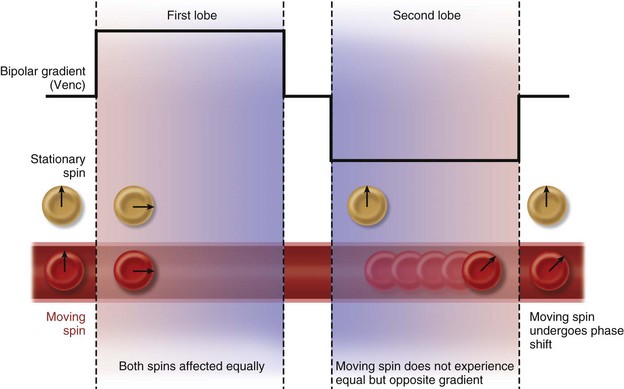
 FIGURE 17-1 Diagram of the effect of bipolar gradients on stationary and moving spins. Venc, velocity encoding value.
FIGURE 17-1 Diagram of the effect of bipolar gradients on stationary and moving spins. Venc, velocity encoding value.
(Modified from Westbrook C, Roth CK, Talbot J. MRI in Practice, 3rd ed. Oxford, Wiley-Blackwell, 2005.)
Flow-Encoding Axes
Flow quantification is performed by prescribing an imaging plane orthogonal to the direction of flow within a vessel. During postprocessing, the borders of the vessel are delineated with a flexible region of interest for each segment of the cardiac cycle. This creates a cross-sectional area for each time point and defines the pixels that contain velocities representing intravascular flow. The spatial mean velocity is then calculated from these pixels and multiplied by the cross-sectional area for each time point in the cardiac cycle (Fig. 17-2). The result is blood flow calculated in milliliters per heartbeat.1
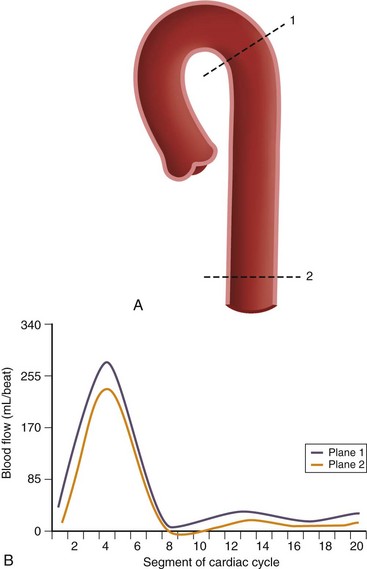
 FIGURE 17-2
FIGURE 17-2Pressure gradients can be estimated with the modified Bernoulli equation, ΔP = 4ν2, where ΔP is the peak pressure gradient in millimeters of mercury and ν is the peak blood flow velocity in meters per second. Unlike flow quantification, phase contrast imaging planes may be prescribed in a parallel or perpendicular orientation with respect to the direction of blood flow to capture the point of peak velocity of flow downstream from a stenosis (Fig. 17-3). It is important to select a relatively high velocity encoding (Venc) value because peak velocities associated with stenotic valves can exceed 5 m/sec.2
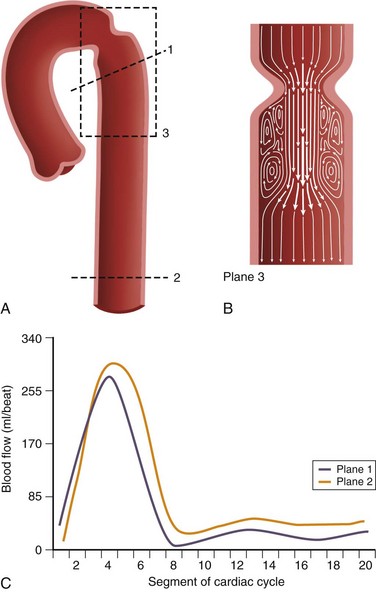
 FIGURE 17-3 A and B, Two-dimensional velocity-encoded cine phase contrast scan planes in the proximal (plane 1) and distal (plane 2) descending thoracic aorta for quantification of collateral blood flow in coarctation of the aorta. Plane 3 is prescribed in the direction of flow to measure peak velocity, which is used to derive the pressure gradient across the stenosis used in the modified Bernoulli equation.11 C, Typical aortic blood flow with two-dimensional velocity-encoded phase contrast MR imaging. Note that the distal blood flow (plane 2) is higher than the proximal flow (plane 1). The area between the curves represents collateral flow.
FIGURE 17-3 A and B, Two-dimensional velocity-encoded cine phase contrast scan planes in the proximal (plane 1) and distal (plane 2) descending thoracic aorta for quantification of collateral blood flow in coarctation of the aorta. Plane 3 is prescribed in the direction of flow to measure peak velocity, which is used to derive the pressure gradient across the stenosis used in the modified Bernoulli equation.11 C, Typical aortic blood flow with two-dimensional velocity-encoded phase contrast MR imaging. Note that the distal blood flow (plane 2) is higher than the proximal flow (plane 1). The area between the curves represents collateral flow.
Velocity Encoding
Phase contrast MRI can be optimized for different velocities of blood flow. The encoding velocity of a given sequence, or Venc, is selected on the basis of the maximum anticipated velocity of the blood flow of interest. The scanner will use this value to adjust the amplitude and duration of the phase contrast bipolar gradients so that a proton moving at the selected Venc value will give rise to a phase shift of 180 degrees. For example, for a Venc value of 100 cm/sec, the range of phase shifts will be adjusted to encode velocities from −100 cm/sec to +100 cm/sec (Fig. 17-4). The lower the Venc value selected, the greater the sensitivity to slower flow but also the stronger the required gradients and the longer the repetition time (TR) of the sequence. An ideal Venc value is slightly greater than the maximum expected velocity.
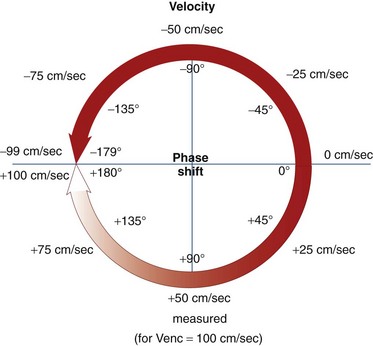
 FIGURE 17-4
FIGURE 17-4Imaging Limitations and Pitfalls
There are some pitfalls to be aware of in employing phase contrast MRI for blood flow quantification. Signal aliasing will occur if the peak velocity of blood flow surpasses the Venc value at any point in the cardiac cycle. This phenomenon takes place because positive velocities that surpass the Venc value will give rise to phase shifts that are interpreted as negative velocities (e.g., a phase shift of 185 degrees will be interpreted as −175 degrees). On phase images, areas of aliasing are easily identifiable: the sudden loss of signal in regions of maximum signal brightness (Figs. 17-5 and 17-6).
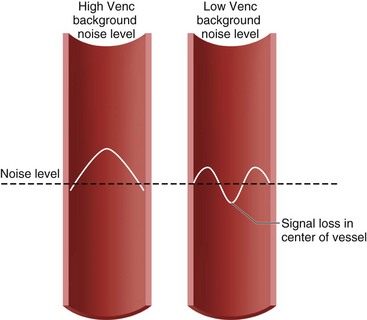
 FIGURE 17-5 Diagram of aliasing with low but not with high velocity encoding value (Venc).
FIGURE 17-5 Diagram of aliasing with low but not with high velocity encoding value (Venc).
(Modified from Westbrook C, Roth CK, Talbot J. MRI in Practice, 3rd ed. Oxford, Wiley-Blackwell, 2005.)
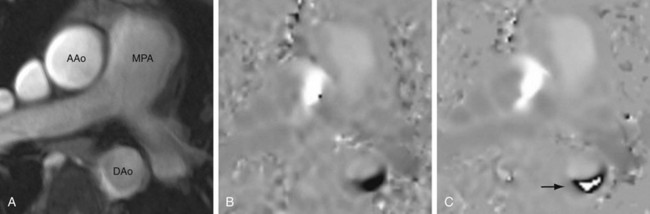
 FIGURE 17-6
FIGURE 17-6Underestimation of velocity and flow can occur if a vessel is not evaluated in a plane orthogonal to the direction of flow or if partial volume averaging occurs. In addition, peak flow velocity downstream of a stenosis, and thus the associated pressure gradient, can be underestimated for two reasons: (1) as the accuracy of peak velocity measurement is dependent on temporal resolution, the value may be underestimated by MRI compared with echocardiography, which has a higher temporal resolution; and (2) the precise, three-dimensional location of the peak velocity downstream from a stenosis may not be included in the two-dimensional phase contrast evaluation.3,4
TECHNIQUES
Technique Description
Valvular Disease
Precise quantification of aortic, pulmonary, and mitral regurgitation has been demonstrated with phase contrast MRI.5–7 Aortic and pulmonary regurgitant volume can be quantified directly, resulting in more accurate and reproducible data than with echocardiography, by which blood flow is estimated on the basis of the apparent size of flow jets, which can be significantly affected by imaging parameters and orientation. The imaging plane is prescribed perpendicular to the direction of blood flow at approximately 1 to 2 cm above the level of the semilunar valve in question (Fig. 17-7). Valvular regurgitant fraction is the ratio of retrograde to antegrade flow across a valve.
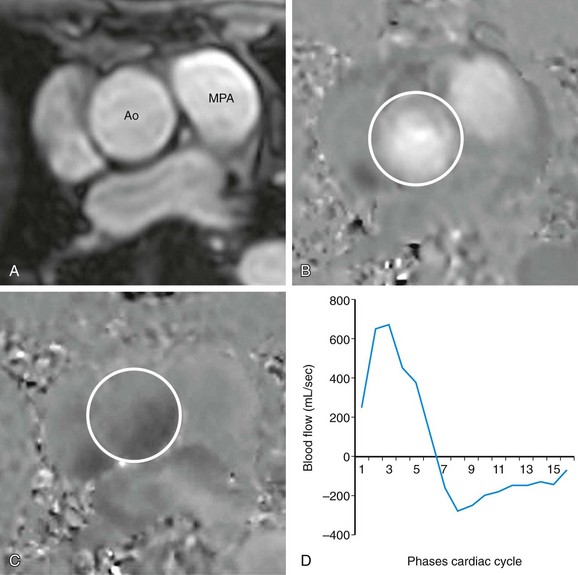
 FIGURE 17-7
FIGURE 17-7


