CHAPTER 50 Magnetic Resonance Imaging in the Postoperative Evaluation of the Patient with Congenital Heart Disease
POSTOPERATIVE ASSESSMENT
A number of MRI techniques are useful to the examination of the anatomy and physiology of the postoperative CHD patient. These techniques are detailed in Chapters 13 to 17. Here, their importance to this population is highlighted.
Cine Magnetic Resonance Imaging
ECG-gated gradient-echo sequences can be employed to provide multiple images throughout the cardiac cycle in prescribed anatomic locations. Display of these images in a cine mode permits visualization of the dynamic motion of the heart and vessels.1–3 Cine MRI techniques, at a minimum, allow assessment of anatomy. More important, such techniques allow qualitative and quantitative assessment of function. Specifically, cine MRI permits quantification of chamber volumes, myocardial mass, and ventricular function. Further, cine MRI allows qualitative assessment of focal and global wall motion abnormalities, qualitative and quantitative assessment of valve disease (including the mechanism and severity of valve regurgitation and the location and severity of valve stenoses), identification and quantification of intracardiac and extracardiac shunts, and visualization of other areas of flow turbulence.
Cine MRI is the principal tool used to quantitatively assess ventricular function. Such techniques, both fast gradient-echo4–7 and balanced steady-state free precession,1,2 have been extensively evaluated and validated.8,9 Briefly, evaluation of function begins with obtaining a series of contiguous cine slices along the short axis of the ventricles, extending from base to apex. The prescription of such slices should be performed from a true four-chamber view at end-diastole to ensure coverage of the entire ventricular mass (Fig. 50-1). These images are played back in a cine loop, and the end-systolic and end-diastolic phases are chosen. The endocardial borders are traced at both time points, and the epicardial borders are traced at one of the two time points (Fig. 50-2). Ventricular volumes are then calculated as the sum of the traced volumes (area × slice thickness). Myocardial mass is calculated as the myocardial muscle volume × 1.05 g/mm3 (density of myocardium). From these data, ventricular end-diastolic volume, end-systolic volume, stroke volume, ejection fraction, myocardial mass, and mass-to-volume ratio can be calculated for both the right and left ventricles. Most computer workstation software packages for cardiac MRI analysis provide semiautomated postprocessing tools to maximize efficiency.
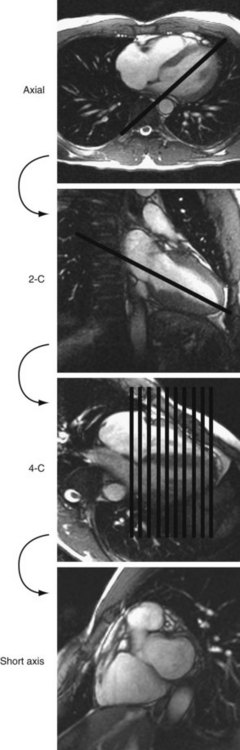
 FIGURE 50-1
FIGURE 50-1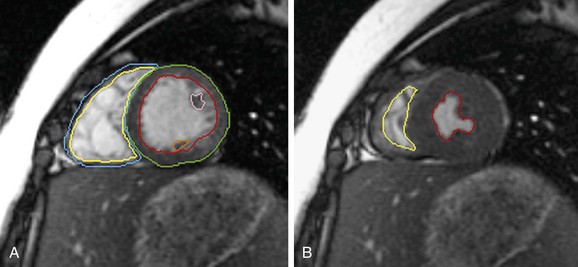
 FIGURE 50-2
FIGURE 50-2Spin-Echo (Black Blood) Imaging
ECG-gated spin-echo sequences (black blood imaging) represent another important tool for imaging in the postoperative CHD patient. Despite providing only static information, black blood imaging has many benefits in this population. It allows assessment of anatomy with thin slices, high spatial resolution, and excellent blood-myocardium and blood–vessel wall contrast (Fig. 50-3). Black blood techniques are superb for evaluation of the spatial relationship between cardiovascular and other intrathoracic structures, such as the chest wall and the tracheobronchial tree. These features hold particular relevance in delineation of complicated postsurgical cardiac anatomy. Such techniques are also less susceptible to artifact from metallic implanted devices, such as stents, coils, occluder devices, clips, and sternal wires, which are commonly seen in the postoperative CHD patient.
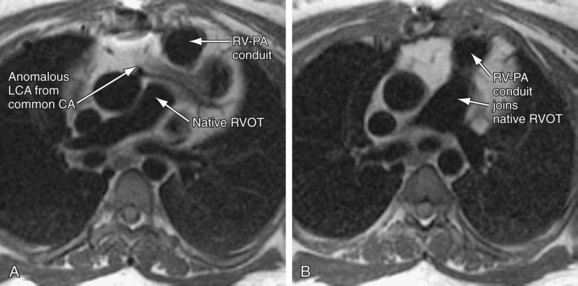
 FIGURE 50-3
FIGURE 50-3Flow Quantification
Electrocardiography-gated gradient-echo sequences with flow-encoding gradients are used to quantify the velocity and flow of blood (Fig. 50-4).10 These sequences are referred to as velocity-encoded cine MRI or phase contrast MRI. Two-dimensional velocity-encoded cine MRI sequences are commonly used in clinical practice. They can be used to quantify cardiac output, pulmonary-to-systemic flow ratio (shunt), valvular regurgitation, differential lung perfusion, and coronary flow reserve. They can be used to observe the location and severity of flow obstruction. In addition, velocity-encoded cine MRI assessment of flow is useful for corroboration of volumetric data obtained with cine imaging to ensure the interpreting physician that the data obtained are accurate.
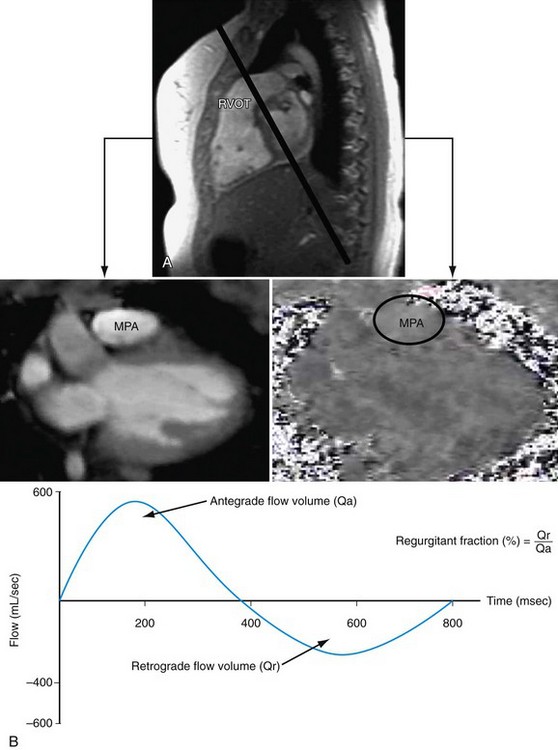
 FIGURE 50-4
FIGURE 50-4Newer velocity-encoded cine MRI sequences allow resolution of velocity vectors in three directions, with spatial coverage of a three-dimensional volume, temporally resolved throughout the cardiac cycle. Such techniques have been coined seven-dimensional flow encoding.11,12 These techniques have the advantage of providing complete spatial and temporal resolution of velocity with a higher signal-to-noise ratio than in two-dimensional methods. Postprocessing tools permit the construction of vector field plots that highlight the intracardiac and intravascular nature of flow. Although they are currently limited by long scan durations, faster imaging techniques will likely allow such methods to reach clinical practice in the near future.
Gadolinium-Enhanced Three-Dimensional Angiography
Three-dimensional magnetic resonance angiography (MRA) sequences are typically not ECG-gated and thus do not allow optimal assessment of intracardiac structures. Regardless, such techniques provide excellent depiction of arterial and venous vascular structures (Fig. 50-5). In the population of postoperative CHD patients, three-dimensional MRA fills a significant diagnostic role. It can be used to diagnose systemic arterial anomalies, such as aortopulmonary collaterals, shunts, vascular rings, and coarctation. It is useful in the diagnosis of pulmonary arterial abnormalities, such as focal and diffuse stenoses and abnormal distal arborization patterns. Three-dimensional MRA methods are also useful for investigation of systemic and pulmonary venous abnormalities, both congenital anomalies and postoperative abnormalities. Finally, three-dimensional MRA is useful for evaluation of the relation between vascular and other thoracic structures. With the development of faster imaging techniques, ECG-gated three-dimensional MRA sequences are becoming more practical, allowing evaluation of intracardiac anatomy and acquisition of time-resolved three-dimensional MRA data sets.13
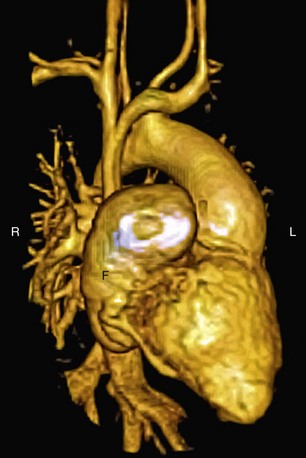
 FIGURE 50-5
FIGURE 50-5Coronary Artery Imaging, Perfusion Imaging, and Myocardial Viability
Coronary artery abnormalities and ischemia are important issues to be investigated in postoperative CHD patients. Not only is this population of patients aging sufficiently to develop atherosclerotic coronary artery disease, they also commonly have congenitally abnormal or postoperatively acquired coronary artery lesions. It is not uncommon to find an anomalous origin or course of the left or right coronary artery, postsurgical coronary obstruction (i.e., after arterial switch for transposition of the great arteries), coronary artery thrombus (Fig. 50-6), or abnormal fistulous connections (i.e., pulmonary atresia with intact ventricular septum and right ventricle–dependent coronary circulation). Identification of such abnormalities is often critical to planning of reintervention or medical management. There is growing evidence to support that myocardial delayed hyperenhancement in a number of subsets of postoperative CHD patients is predictive of poor outcome, including patients with tetralogy of Fallot (Fig. 50-7).14,15 Delayed hyperenhancement has been observed in other postoperative patients with CHD as well, the significance of which is being explored and elucidated.16,17 In summary, although it is still not as robust as routine coronary artery angiography with x-ray fluoroscopy or ECG-gated CT angiography at investigating distal coronary artery lesions, MRI can image proximal coronary arteries well,18–21 evaluate myocardial perfusion and viability,22–26 and allow stress testing,27–30 all noninvasively without exposure to contrast agents and ionizing radiation.
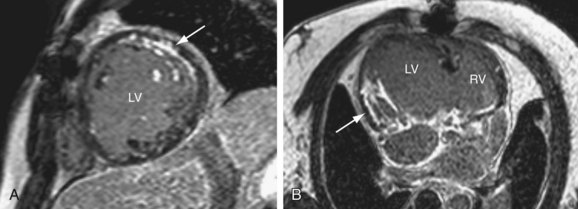
 FIGURE 50-6
FIGURE 50-6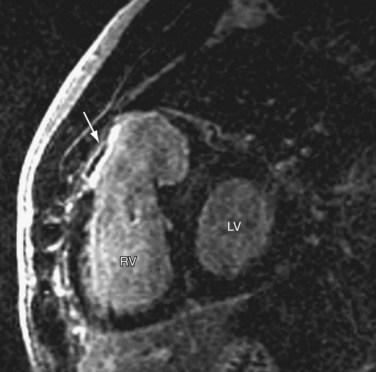
 FIGURE 50-7
FIGURE 50-7


