CHAPTER 57 Magnetic Resonance Imaging of Myocardial Viability
Heart failure is a complex clinical syndrome with high hospitalization and mortality rates. The incidence of heart failure approaches 10 per 1000 in the population older than 65 years.1 The most common etiology of heart failure in developed countries is coronary artery disease. In patients with left ventricular (LV) dysfunction, it is of great therapeutic and prognostic importance to differentiate irreversibly damaged scarred myocardium, dysfunctional but viable myocardium (hibernating or stunned), and LV dysfunction from causes not related to coronary artery disease. The assessment of myocardial viability is important to guide the management of patients with ischemic LV dysfunction when clinicians must weigh the risks and benefits of coronary revascularization in regard to the increased perioperative morbidity and mortality in this patient population.2,3
The meta-analysis by Allman and colleagues4 assessed the prognostic value of viability assessment across various nuclear and echocardiographic techniques. Determining the presence and extent of myocardial viability is crucial in guiding clinical decision making and influencing patient outcomes. Patients with significant viability assigned to be treated medically had higher rates of cardiac mortality (16% vs. 3.2 % per year) and nonfatal myocardial infarction (MI) (12.2% vs. 6 % per year) than patients who were assigned to undergo coronary revascularization. In patients without significant myocardial viability, there was no difference in annual mortality or nonfatal MI rates between coronary revascularization and medical therapy (7.7% vs. 6.2% and 10.2% vs. 8%).4 These findings underscore the importance of noninvasive assessment of viability in guiding appropriate treatment decision making.
VIABILITY DEFINITIONS
Stunned and hibernating myocardium can benefit from restoration of blood supply. Rahimtoola5 first reported the process of myocardial hibernation, and it was then observed that LV dysfunction resulting from myocardial hibernation is not an irreversible process. The process of myocardial hibernation is a dynamic process that involves a continuum of downregulation of myocyte metabolism, reduction in contractile elements, and dedifferentiation of myocardial cells with preserved cell membrane integrity. The following processes have been observed in hibernating myocardium: loss of sarcomeres, sarcoplasmic reticulum, and T tubules; intracellular buildup of glycogen; atrophic mitochondria; accumulation of extracellular matrix and fibrosis; and expression of fetal proteins.6
MAGNETIC RESONANCE IMAGING ASSESSMENT OF MYOCARDIAL VIABILITY
Several MRI techniques exist to assess myocardial viability. Common clinical techniques include assessment of LV end-diastolic wall thickness on resting cine MRI, myocardial contractile reserve and ischemia by dobutamine stress MRI (dobutamine MRI), and transmural extent of MI by contrast-enhanced myocardial delayed enhancement (MDE) imaging. Other MRI techniques, such as quantification of myocardial contractile reserve with MRI tagging7,8 and MR spectroscopy for assessment of high-energy phosphates metabolism (e.g., quantification of concentration and ratio of adenosine triphosphate and phosphocreatine using 31P spectroscopy within a small volume of myocardium), are currently not in wide clinical use and are beyond the scope of this chapter.9,10
Wall Thickness
In the presence of extensive chronic MI, wall thinning develops in the infarct zone because of infarct resorption and fibrotic contracture. Although autopsy studies have shown that wall thinning is frequently associated with transmural scar,11,12 end-diastolic wall thickness (EDWT) measured in millimeters has limited prediction for functional recovery after revascularization, which serves as the most common surrogate reference method for myocardial viability. Baer and coworkers13 compared resting MRI with 18FDG-PET in 35 patients. Regions with EDWT less than 5.5 mm had significantly reduced 18FDG uptake compared with regions with thickness 5.5 mm or greater that had preserved 18FDG uptake. The same investigators also tested the predictive value of EDWT for functional recovery after revascularization. A EDWT cutoff of 5.5 mm had 94% sensitivity, but only 52% specificity for predicting segmental functional recovery after revascularization.14
The low specificity of LV wall thinning can be attributed to the fact that myocardial segments even with preserved wall thickness can have substantial transmural scar. In addition, EDWT is a structural variable that does not assess physiologic response of the myocardium, and there is a wide variation of EDWT among individuals and among different myocardial segments in the same individual.15 Kim and Shah15 showed that regional wall thinning may occur early after MI even in the absence of transmural necrosis, and that the thinned myocardium can still improve its contractile function.
Dobutamine Magnetic Resonance Imaging Contractile Reserve
Improvement in wall thickening or contractile reserve in response to inotropic challenge such as a low-dose dobutamine infusion (5 to 15 µg/kg/min) has been well validated for assessment of myocardial viability in echocardiography and MRI literature.14,16–20 There are several advantages of MRI over the conventional echocardiography for detecting contractile reserve. Widely used cine steady-state free precession provides excellent spatial resolution and tissue contrast between the blood pool and LV myocardium. In contrast to echocardiography, which is limited by acoustic windows, MRI is able to provide multiplanar image acquisition for improved volumetric coverage of the heart. The quantification of LV volumes, mass, and ejection fraction with MRI does not require any geometric assumptions and is highly reproducible.21
Schmidt and colleagues22 assessed resting EDWT (5.5 mm cutoff), dobutamine-induced wall thickening of greater than 2 mm, and presence of normalized 18FDG uptake greater than 50% on PET in 40 patients with chronic MI to predict segmental functional recovery. The sensitivity and specificity for segmental functional recovery were 100% and 53% for resting EDWT 5.5 mm or greater alone, 96% and 87% for dobutamine-induced contractile reserve, and 100% and 73% for preserved 18FDG (>50%) uptake. These findings indicate that dichotomizing a threshold value of resting EDWT or 18FDG uptake is less accurate than the physiologic assessment of low-dose dobutamine challenge. This point is supported further by a study reported by Wellnhofer and associates,20 which showed higher specificity of dobutamine MRI compared with transmural extent of late hyperenhancement on MDE imaging to predict functional recovery, especially with 1% to 74% transmural extent of late hyperenhancement.
Contractile response during low-dose dobutamine challenge is specific, yet is only moderately sensitive in detecting segmental viability. Kaandorp and coworkers23 reported a weighted mean sensitivity and specificity for predicting functional recovery of 73% and 83% after pooling nine previously published dobutamine MRI studies. The relatively low sensitivity of dobutamine MRI can be attributed to the fact that in the presence of severe coronary stenosis, viable myocardial segments fail to show augmentation of segmental thickening because of rapid development of ischemia even with low dobutamine doses. We choose to infuse low-dose dobutamine using 5-minute per stage protocol. This prolonged infusion allows building up of the inotropic effects of the dobutamine, and the resultant display of augmentation of segmental thickening may enhance the sensitivity in detection of segmental viability.
Hyperenhancement on Myocardial Delayed Enhancement Imaging
The basis for development of MDE imaging was an observation that the differential between normal and infarcted myocardium can be accentuated by the use of gadolinium-chelate contrast agents on T1-weighted images.24 Gadolinium shortens the T1 relaxation time of tissues with increased gadolinium content. Nevertheless, the limitation in image quality had restricted the clinical application of contrast-enhanced MRI until recent years. The proposed mechanism of hyperenhancement on MDE (also known as late gadolinium enhancement) is related to a relatively large molecular size of conventional extracellular gadolinium-chelate contrast agents that is made metabolically inert by the chelation and unable to cross the cell membrane of a normal myocyte. When the cell membrane is damaged (e.g., acute MI), or if there is an increase in the extracellular space between myocytes (e.g., acute interstitial edema or chronic fibrosis), there is accumulation of gadolinium-chelate contrast agent in the extracellular space, and its washout is delayed after the injection (Fig. 57-1).
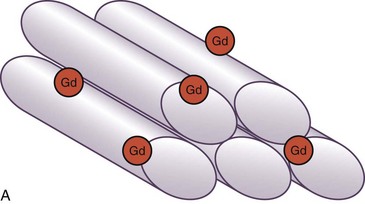
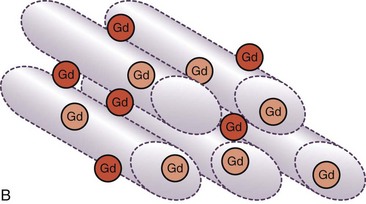
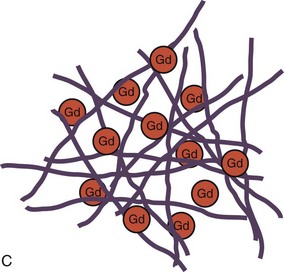
 FIGURE 57-1
FIGURE 57-1


