Magnetic resonance (MR) imaging offers a noninvasive tool for diagnosis of primary and metastatic pelvic tumors. The diagnosis of a pelvic metastatic lesion implies an adverse prognosis and dictates the management strategies. Knowledge of normal MR imaging anatomy of the pelvis and the signal characteristics of normal and abnormal structures is essential for accurate interpretation of pelvic MR imaging. This article reviews imaging manifestations of nodal, visceral, and musculoskeletal metastatic lesions of the pelvis along with current and evolving MR imaging techniques.
Key points
- •
Lymph node involvement signifies an adverse prognosis and modifies the treatment strategies. The number and regions of affected pelvic nodes directly influence the survival rate.
- •
Superior soft tissue resolution of magnetic resonance (MR) imaging aids in detection of metastatic lesions to visceral organs and detects nonpalpable lesions of the prostate, penis, and testes.
- •
Disseminated tumors commonly seed pelvic recesses lined by parietal peritoneum, followed by accumulation of increasing amounts of ascites in the bilateral paravesical recesses.
- •
MR imaging offers better characterization of musculoskeletal metastasis compared with computed tomography and conventional radiography.
- •
With diffusion-weighted imaging and nanoparticle-enhanced MR imaging there is an impending paradigm shift from structural to functional imaging.
Introduction
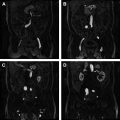
The pelvis is a common site for primary and metastatic tumors. Diagnosis of pelvic metastatic lesions is a crucial step in the staging of primary cancer because it implies an adverse prognosis. Magnetic resonance (MR) imaging is a noninvasive imaging tool for diagnosis of pelvic metastasis based on its multiplanar imaging capability and excellent soft tissue resolution. In addition, MR imaging can also differentiate between different tissue elements including characterization of vascular and nonvascular structures without contrast. Knowledge of basic MR signal characteristics of normal ( Figs. 1–5 , Table 1 ) and abnormal structures is essential for accurate interpretation of pelvic MR imaging. This article provides a concise overview of nodal, visceral, and musculoskeletal metastatic lesions affecting the pelvis and their MR imaging characteristics.





| Organ | T1 Appearance | T2 Appearance |
|---|---|---|
| Bladder wall | Intermediate signal | Low signal intensity |
| Testicles | Homogeneous intermediate signal intensity | High signal intensity relative to skeletal muscle |
| Epididymis | Isointense to the testis | Lower signal intensity than the testis |
| Tunica albuginea | Low signal intensity | Low signal intensity |
| Corpora cavernosa and spongiosa | Intermediate signal intensity | Corpus spongiosum shows homogeneous high signal intensity Corpora cavernosa may have a heterogeneous signal intensity |
| Prostate | Low to intermediate signal intensity | Glandular tissue normally shows high signal intensity, whereas fibromuscular stromal elements have low signal intensity |
| Bone marrow | Hematopoietic marrow equal to or slightly higher than muscle | The same as T1 |
| Muscle | Intermediate between fat and cortical bone | Intermediate between fat and cortical bone |
Introduction
The pelvis is a common site for primary and metastatic tumors. Diagnosis of pelvic metastatic lesions is a crucial step in the staging of primary cancer because it implies an adverse prognosis. Magnetic resonance (MR) imaging is a noninvasive imaging tool for diagnosis of pelvic metastasis based on its multiplanar imaging capability and excellent soft tissue resolution. In addition, MR imaging can also differentiate between different tissue elements including characterization of vascular and nonvascular structures without contrast. Knowledge of basic MR signal characteristics of normal ( Figs. 1–5 , Table 1 ) and abnormal structures is essential for accurate interpretation of pelvic MR imaging. This article provides a concise overview of nodal, visceral, and musculoskeletal metastatic lesions affecting the pelvis and their MR imaging characteristics.
| Organ | T1 Appearance | T2 Appearance |
|---|---|---|
| Bladder wall | Intermediate signal | Low signal intensity |
| Testicles | Homogeneous intermediate signal intensity | High signal intensity relative to skeletal muscle |
| Epididymis | Isointense to the testis | Lower signal intensity than the testis |
| Tunica albuginea | Low signal intensity | Low signal intensity |
| Corpora cavernosa and spongiosa | Intermediate signal intensity | Corpus spongiosum shows homogeneous high signal intensity Corpora cavernosa may have a heterogeneous signal intensity |
| Prostate | Low to intermediate signal intensity | Glandular tissue normally shows high signal intensity, whereas fibromuscular stromal elements have low signal intensity |
| Bone marrow | Hematopoietic marrow equal to or slightly higher than muscle | The same as T1 |
| Muscle | Intermediate between fat and cortical bone | Intermediate between fat and cortical bone |
Lymph node metastasis
In most patients with known pelvic malignancies, presence of nodal disease signifies adverse prognosis and dictates treatment strategies. The number and regions of the pelvic nodes involved affect the nodal (N) and metastasis (M) staging of the tumor and also influence the survival rate. Understanding the lymphatic drainage pathways and MR diagnostic criteria of abnormal nodes can help in the evaluation of pelvic lymph node metastasis.
Pelvic Lymphatic Metastatic Pathways
The primary lymphatic drainage in the male pelvis includes 4 pathways: (1) the anterior route, draining lymph from the anterior wall of the bladder to the internal iliac (hypogastric) nodes; (2) the lateral route, draining lymph from pelvic organs to the external iliac nodal group; (3) the internal iliac (hypogastric) route, draining lymph to the junctional nodes located at the junction between the internal and external iliac vessels; and (4) the presacral route, draining lymph to the common iliac nodes. To a great extent, the location of the primary tumor (bladder, prostate, testes, and penis) and integrity of the draining lymphatics determine which pathway is predominantly affected. The location of the involved lymph nodes can be attributed to N or M stage; for example, inguinal nodes are considered as regional metastasis for penile cancer but distant metastasis for prostate cancer. Familiarity with these lymphatic metastatic pathways is crucial for pelvic node evaluation.
Prostate Cancer
The lymphatic drainage of prostate cancer involves the obturator, presacral, hypogastric, and external iliac nodes and further to the common iliac and para-aortic nodes. The main drainage pathway is the lateral route, which involves nodes located along the lateral aspect of the external iliac artery, and the sentinel nodes are the obturator nodes. From there, the tumor may further spread to the nodes located medial and posterior to the external iliac vein. The second most common pathway is the internal iliac route, via the nodes located along the visceral branches of the internal iliac vessels, and the corresponding sentinel nodes are located at the junction of the internal and external iliac vessels. Following therapeutic irradiation of the prostate or radical prostatectomy, recurrent metastatic disease is most often seen in extrapelvic nodes. The survival rate depends on the number of positive nodes. The 10-year disease-free survival in cases of solitary nodal involvement is 70%, compared with 49% for multiple (more than 5) nodes.
Penile Cancer
The lymph node metastasis of penile cancer commonly involves the nodes in the superficial and deep inguinal regions, and subsequently the pelvic lymph nodes associated with ipsilateral iliac vessels and obturator fossa are also affected. The saphenofemoral junction node is the sentinel node for penile cancer. Greater number of metastatic nodes, bilateral disease, and deep pelvic nodal metastases adversely affect prognosis. The mortality increases from 25% in cases of low-volume inguinal metastases to 75% in patients with more than 2 nodes. In patients with penile carcinoma, nodal metastases at the time of diagnosis can be seen in 22% to 61% of patients.
Testicular Cancer
Testicular cancer spreads via the para-aortic pathway, with lymphatic drainage following the gonadal vessels to the retroperitoneum, whereas metastases in pelvic nodes are rare except in epididymal cancer. As the volume of the tumor increases, the metastasis may further spread from retroperitoneal nodes to the common iliac, internal iliac, and external iliac nodes. More importantly, because of disruption of the normal lymphatic drainage pathways after orchiectomy, the pelvic and inguinal nodes should be assessed as regional nodes. The spread of testicular cancer is most commonly by means of lymphatic metastasis. The evaluation of nodal status dictates the of postorchidectomy radiation and helps in assessing treatment response. MR imaging is especially useful in this regard because patients with seminomas are often young adults and have a good 5-year survival rate (>80%).
In testicular cancer, unlike many other malignancies, the lymph nodes should be measured by calculating the maximum diameter of the lymph node as opposed to the short-axis of the lymph node.
Bladder Carcinoma
Bladder carcinoma commonly spreads via a pelvic pathway and the specific sites of primary tumors determine the pathway. For tumors located in the fundus of the bladder, the most common sites of metastasis are the obturator and internal iliac nodes; for upper and lower lateral wall tumors, the external iliac nodes are predominantly affected; and for bladder neck cancers, node metastasis spreads from the presacral nodes to the common iliac nodes. However, radical cystectomy for bladder cancer can change the pathways and, in such circumstances, clinicians should carefully evaluate the common iliac and para-aortic nodes. The metastatic lymph nodes below the level of the common iliac vessels are categorized as regional metastasis, whereas the nodes above the level of common iliac vessels are categorized as distant metastasis. Similar to penile neoplasm, as the number of nodes involved increases, the survival rate of bladder cancer decreases. Three-year survival in node-negative patients is approximately 70%; in patients with solitary positive node it is approximately 50%, and it is reduced to approximately 25% if multiple nodes are involved.
Rectal Cancer
Rectal lymph drainage follows 3 pathways depending on the sites of primary tumors: (1) upper rectum, to the inferior mesenteric nodes followed by the para-aortic nodes; (2) middle rectum, to the obturator and hypogastric nodes; (3) lower rectum, to the inguinal nodes.
In T3 rectal tumors, survival in lymph node–negative patients is approximately 70%, compared with 35% in lymph node–positive patients, and survival in patients with 1 to 3 nodes involved is significantly better than in those with more than 3 nodes.
Metastatic pelvic side wall (PSW) nodes on MR imaging represent a more advanced disease state in rectal cancer ( Fig. 5 ). The obturator fossa is the predominant site for PSW node metastasis. Among patients undergoing primary surgery, PSW node involvement suspected on MR imaging is associated with worse 5-year disease-free survival compared with no suspected PSW node involvement: 31% versus 76%.
Diagnostic Criteria
Multiplanar MR imaging has shown an accuracy of 90%, a positive predictive value of 94%, and a negative predictive value of 89% in the detection of nodal metastasis in bladder and prostate cancer. For conventional MR imaging, the morphologic criteria, including size, shape, contour, fatty hilum, signal abnormalities, and location, are currently followed in clinical practice ( Table 2 ).
| Criteria | Benign | Malignant |
|---|---|---|
| Shape | Ovoid or elongated | Round or spherical |
| Conture | Smooth | Irregular/lobulated/speculated |
| Signal abnormality | Homogenous on T2WI | Heterogeneous on T2WI |
| Necrosis | Necrosis (in tuberculosis, fungal infection and cavitating node syndrome, after therapy) | Central necrosis |
| Fatty hilum | Preserved | Loss |
| Enhancement | Homogeneous | Heterogeneous, similar to the primary tumor |
| Location | Scattered distribution | Clustered distribution |
Nodal size
Nodal size is the main criteria to distinguish between malignant and benign change in lymph nodes. Lymph nodes with a maximum short diameter of no more than 10 mm are generally accepted as benign. However, this criterion has 2 main limitations: the proportion of nodes that harbor metastases from urogenital cancers is usually smaller; and nodal hyperplasia also can cause volume increase of lymph nodes. When using a common size standard of 10 mm, a high false-negative rate caused by the involved nodes of normal size may weaken the diagnostic accuracy of lymph node metastasis on MR imaging in patients with prostate cancers. If the size standard decreases to 6 mm, a higher sensitivity (78%) and specificity (98%) can be obtained. Hence, some investigators have proposed that the size criterion should be altered according to the location of the node and the primary tumor. Grubnic and colleagues advocate that lymph nodes with a maximum short-axis diameter of more than 6 mm in the pelvis and 5 mm in the retroperitoneum should be considered abnormal. Vinnicombe and colleagues suggested that the upper limit of the maximum short-axis diameter for normal lymph nodes in patients with testicular tumors should be 10 mm for the external iliac region, 9 mm for the common iliac region, and 7 mm for the internal iliac region. Koh and colleagues suggested a maximum short-axis diameter of 8 mm in patients with testicular cancer for retroperitoneal lymph nodes. Gualdi and colleagues and Brown and colleagues suggested that lymph node size was not a useful criterion. Thin-slice MR imaging of 3-mm to 4-mm slice interval and 0.4-mm to 0.5-mm interslice gap could detect a larger number of lymph nodes than a 5-mm slice interval and 3-mm interslice gap, suggesting the importance of protocol selection in the clarification of metastasis. In rectal cancer, for instance, MR imaging is able to detect perirectal and presacral lymph nodes with sizes ranging from 1 to 5 mm.
Shape and contour of the nodes
Shape and contour of the nodes can be useful in the distinction of metastasis from benign nodes. Most benign nodes are ovoid, as opposed to malignant nodes, which tend to have a rounded shape, although combining the criteria of size and shape does not improve the accuracy of radiological assessment of urogenital pelvic cancers compared with using size as the single criterion. Nodal involvement might lead to an irregular node border if extracapsular extension of metastatic disease is present ( Fig. 6 ), although this sign is rarely observed in small nodal metastases.
Signal abnormalities
Signal abnormalities of involved lymph nodes are mainly caused by altered nodal composition caused by tumor deposits. Metastatic nodes show low signal intensity that is usually a little higher than that of normal vessels on T1-weighted images and intermediate signal intensity on T2-weighted images. However, signal intensities of malignant nodes often do not differ from those of benign nodes on T1-weighted and T2-weighted images because T1 and T2 relaxation times of metastatic and normal nodes overlap considerably. Heterogeneous signal inside nodes on T2-weighted images, especially necrosis, is more likely to be malignant than homogeneous nodes ( Fig. 6 ). Internal abnormalities such as loss of fatty hilum, calcifications and accumulations of fat or fluid may be helpful for identifying nodal metastases, which may resemble a primary malignancy in the signal intensity on MR imaging. Nodal calcifications may be seen in metastasis from bladder cancer, although it is not a reliable sign because it can also be seen in benign inflammatory disease such as tuberculosis. Cystic appearance resulting from central necrosis is observed in metastatic nodes, especially from the testicular nonseminomatous germ cell tumors, which have high signal intensity on T2-weighted images. Noncystic but large metastatic nodes can appear heterogeneous, with a central low-density component that can be caused by necrosis, but this finding can also be seen in tuberculosis and various fungal infections. Such a central zone of necrosis is only rarely found in metastatic retroperitoneal and pelvic nodes. This finding can be further shown by administration of contrast agents. Inhomogeneous enhancement with an enlarged size or similar enhancement with primary tumor strongly implies malignant infiltration in nodes. Moreover, on enhanced scan, a signal intensity time curve may be helpful for detecting nodal involvement in normal-sized nodes.
Location of lymph node
The location of lymph nodes can aid in resolving the ambiguities regarding the metastasis. Nodes that are located along the pathway of lymphatic drainage from a primary tumor, when borderline in size or when they have had a recent increase in size, are more likely to contain metastatic infiltration. The distribution of cluster nodes, even normal-sized nodes, is also considered suspicious for metastasis.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


