Penile cancer is a rare neoplasm that, although rare in the developed world, has devastating physical and psychological consequences for the patient. Novel MR imaging techniques such as lymphotropic nanoparticle-enhanced MR imaging may help identify metastatic lymph node disease. This article reviews the normal penile anatomy and MR imaging techniques and features of primary and metastatic penile cancer. Recent advances in penile cancer imaging are discussed.
Key points
- •
Penile cancer, although rare in the developed world, has devastating physical and psychological consequences for the patient.
- •
MR imaging accurately delineates the penile anatomy and is the imaging modality of choice of accurate local staging of primary penile cancer.
- •
Novel MR imaging techniques such as lymphotropic nanoparticle-enhanced MR imaging may help identify metastatic lymph node disease.
Introduction
Penile cancer is a rare neoplasm with devastating physical and psychological consequences for patients. There is a wide regional variation in the incidence of penile cancer throughout the world ranging from less than 1 case per 100,000 men in Europe and the United States, to 8.3 cases per 100,000 in Brazil, to even higher in Uganda. In the United States, it is estimated that there will be 1640 new cases of penile cancer and 320 cancer-related deaths in 2014. Penile cancer tends to be a disease of older men. There is an abrupt increase in incidence in men aged approximately 60 years and the incidence peaks in men aged 80 years.
This article reviews the normal penile anatomy, MR imaging techniques for evaluation of the penis, and MR imaging features of primary and metastatic penile cancer. Recent advances in penile cancer imaging are discussed.
Introduction
Penile cancer is a rare neoplasm with devastating physical and psychological consequences for patients. There is a wide regional variation in the incidence of penile cancer throughout the world ranging from less than 1 case per 100,000 men in Europe and the United States, to 8.3 cases per 100,000 in Brazil, to even higher in Uganda. In the United States, it is estimated that there will be 1640 new cases of penile cancer and 320 cancer-related deaths in 2014. Penile cancer tends to be a disease of older men. There is an abrupt increase in incidence in men aged approximately 60 years and the incidence peaks in men aged 80 years.
This article reviews the normal penile anatomy, MR imaging techniques for evaluation of the penis, and MR imaging features of primary and metastatic penile cancer. Recent advances in penile cancer imaging are discussed.
Anatomy
The anatomy of the penis has important implications for the diagnosis and treatment of penile cancer. The penis can be divided into root and body. The root of the penis is located in the superficial perineal pouch and is the primary fixation point. The body of the penis is composed of three tubular endothelium-lined cavernous structures: paired corpora cavernosa, located on the dorsolateral aspect of the penis, and a single corpora spongiosum located in the midline ventrally ( Fig. 1 ). The corpus spongiosum contains the urethra and extends anteriorly to form the glans penis. The three corpora of the penis are covered by three connective tissue layers. The innermost layer is fibrous tunica albuginea. The middle layer is the Buck fascia, a fibrous layer that surrounds the corpora cavernosa and separates them from corpora spongiosum. External to this is a layer of loose connective tissue that is covered by dartos fascia.
MR imaging
Patient positioning is paramount in MR imaging of the penis. Patient is imaged in a supine position. To elevate the scrotum and penis, a folded towel is placed between the patient’s legs. The penis is taped to the abdomen in a dorsiflexed position to prevent movement and pulsation artifacts. A surface coil is placed on the penis to improve signal-to-noise ratio.
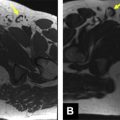
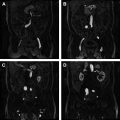
Scardino and colleagues suggested that MR imaging with artificial erection, achieved by injecting 10 μg of prostaglandin E1 into the corpus cavernosum, provides a more robust local staging of the penile cancer. Artificial erection is routinely used at the authors’ institute for MR imaging of the penis. However, this is avoided if there is large and painful penile tumor because of the increased risk of priapism. The MR imaging sequences used are (1) T1-axial images of the pelvis, which provide an overview of the pelvis and lymph nodes and (2) T2-axial, sagittal, and coronal images of the penis ( Box 1 ). Gadolinium-enhanced sequences are not routinely used at the authors’ institute. The three corpora of the penis demonstrate intermediate T1 and high T2 signal on MR imaging. Relative to the corpus spongiosum, the muscular wall of the urethra appears hypointense on both T1-weighted and T2-weighted sequences. Tunica albuginea, Buck fascia, and dartos fascia show low signal intensity on all MR imaging sequences. Tunica albuginea and Buck fascia cannot reliably be differentiated on MR imaging and appear as a hypointense rim of tissue around the corpora. T2-weighted imaging demonstrates a greater degree of contrast between the corpora and tunica albuginea. MR imaging appearances of normal penis are summarized in Table 1 and illustrated in Fig. 2 .
Adequate patient positioning.
Artificial erection: injection of 10 μg of prostaglandin E1 into the corpus cavernosum.
| MR imaging Acquisition Parameters a | TR | TE | FOV |
|---|---|---|---|
| T1 Axial Pelvis | 679 | 12 | 400 b |
| T2 Axial Penis | 5720 | 97 | 350 |
| T2 Sagittal Penis | 3750 | 100 | 250 |
| T2 Coronal Penis | 3750 | 100 | 250 |
Abbreviations: FOV, field of view; TE, echo time; TR, repetition time.
a MR imaging acquisition parameters at the authors’ institute.
b Variable based on patient body habitus.
| T1-Weighted MR Imaging | T2-Weighted MR Imaging | |
|---|---|---|
| Dartos fascia | Hypointense | Hypointense |
| Tunica albuginea and Buck fascia | Hypointense | Hypointense |
| Muscular wall of the urethra | Hypointense a | Hypointense a |
| Corpora cavernosa and corpus spongiosum | Intermediate | High signal |
MR imaging of penile cancer
Primary Tumor Imaging
Most penile cancers are squamous cell carcinomas (SCCs). Other reported histologic types of penile malignancies consist of basal cell carcinoma, melanoma, sarcoma, and metastatic lesions. Moreover, several histologic subtypes of SCC have been described, each with unique clinicopathologic characteristics and outcome features. The most common histologic subtype of penile carcinoma is the usual-type SCC. Most penile tumors originate from the mucosal surface extending from the preputial orifice to the meatus urethralis. Tumors arising from the glans penis are more common than are those involving the foreskin or the sulcus. A recent study of about 5000 cases of invasive penile carcinoma showed that the primary site of disease was the glans penis in 34.5% of cases, prepuce in 13.2%, shaft in 5.3%, and overlapping in 4.5%, with primary site unspecified in 42.5% of cases. MR imaging is the most sensitive imaging modality for local staging of penile cancer because of its exceptional soft-tissue resolution, multiplanar capability, and excellent spatial resolution in the assessment of superficial structures. On MR imaging, primary penile cancers usually appear as solitary, ill-defined, and infiltrating mass lesions that are hypointense relative to the adjacent corpora on both T1-weighted and T2-weighted images. MR imaging enables accurate assessment of the local extent of the penile lesion, depth of tumor invasion, and involvement of tunica albuginea and other adjacent structures, including corpora, urethra, or scrotal skin. The international tumor node metastasis (TNM) staging system for penile cancer was last updated in 2009 and is used for staging the primary tumor ( Fig. 3 , Table 2 ). MR imaging and histology appearances of various T stages of penile cancer are illustrated in Figs. 4–7 .