CHAPTER 40 Magnetic Resonance Imaging of the Aorta and Left Ventricular Function in Inherited and Congenital Aortic Disease
Intrinsic aortic wall abnormalities have been described in inherited connective tissue disorders such as Marfan syndrome and bicuspid aortic valve disease, but recent reports indicate similar aortic involvement in patients with classic congenital heart disease (CHD) entities, such as coarctation of the aorta, tetralogy of Fallot, and transposition of the great arteries, suggesting a degenerative process that results in structural weakness of the aortic wall.1,2 The aortic media consists of smooth muscle and an extracellular matrix that is composed of ground substance, in which elastic fibers and collagen are embedded in a hydrated gel comprising glycosaminoglycans, proteoglycans, and adhesive glycoproteins.1 Smooth muscle cells govern vasodilation and vasoconstriction, collagen provides inert aortic wall strength (stiffness), and elastin—with its low elastic modulus—is readily deformable, permitting phasic distention and recoil in response to pulsatile flow.1 Current focus on the origin of aortic wall abnormalities has shifted toward these specific medial constituents and their crucial role in the structural and functional integrity of the aorta in affected groups of patients.1
In prototypical diseases such as Marfan syndrome and bicuspid aortic valve disease, loss of fibrillin 1 microfibrils has been reported to dissociate smooth muscle cells from the medial matrix components, resulting in accelerated cell death and matrix disruption (Fig. 40-1).2 Matrix metalloproteinases, endogenous enzymes that degrade matrix components, become activated in fibrillin 1–deficient tissues, degrading the structural support of the aorta.2 Similar focal abnormalities within the aortic media have recently been described in coarctation of the aorta, tetralogy of Fallot, and transposition of the great arteries.1 Whether these aortic wall changes result from an intrinsic medial abnormality or are secondary to hemodynamic states before and after surgical repair (or both) is unknown.1 Whatever the etiology of aortic wall disease given this heterogeneity, aortic dilation and reduced aortic elasticity will evolve when loss of structural support of the aortic wall progresses.1,2
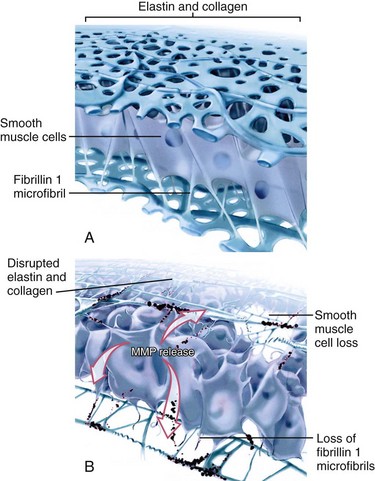
 FIGURE 40-1
FIGURE 40-1With advancing age, ascending aortic elastic fibers will fragment, collagen and ground substance will increase, and the number of smooth muscle cells will decrease.1,3 In addition, arterial hypertension, atherosclerosis, and other cardiovascular risk factors such as smoking, hypercholesterolemia, and diabetes may lead to atheroma formation, which is associated with similar degenerative processes in the extracellular matrix and the vasa vasorum.4 Therefore, the negative sequelae related to aging and numerous cardiovascular risk factors will have a superimposing impact on already existing aortic wall abnormalities.
Both reduced elasticity and dilation of the aorta have a detrimental effect on aortic valve function, especially if the aortic valve is already structurally malformed by being bicuspid or quadricuspid.5,6 As aortic valve opening occurs in concert with root expansion during the beginning of systole, aortic elasticity is crucial for aortic valve dynamics.5,6 Decreased aortic root elasticity increases leaflet stress and therefore predisposes to aortic valve dysfunction.5,6 Aortic dilation contributes to aortic valve dysfunction by loss of coaptation of the aortic valve leaflets.2,5 Moreover, with reduced aortic elasticity, the cushioning windkessel effect of the aorta is impaired. This leads to increased systolic blood pressure and pulse pressure, which in turn will increase myocardial oxygen demand by increasing LV afterload.7 Arterial stiffening is also associated with impaired coronary perfusion, the presence of coronary artery disease, and LV dysfunction.8
As life expectancy of patients with CHD has much improved during the past decades, adult cardiologists will be increasingly confronted with the challenge of concomitant aortic sequelae. Therefore, noninvasive monitoring of aortic dimensions and elasticity, in conjunction with aortic valve competence and LV function, is clinically highly desirable in patients with potential aortic wall abnormalities. Echocardiography is widely used for routine assessment of the aortic root, aortic valve, and ventricular function, but it does not permit evaluation of the entire aorta.4 Magnetic resonance imaging (MRI) provides advantages such as unlimited field of view within the entire thorax for accurate and reproducible assessment of aortic and cardiac anatomy and function.5,9,10
MARFAN SYNDROME
Prevalence and Epidemiology
Marfan syndrome is a heritable connective tissue disorder resulting in a highly variable degree of premature aortic medial degeneration with a high risk of progressive aortic dilation and subsequent aortic dissection or rupture.11,12 Marfan syndrome is caused by a mutation of the FBN1 gene on chromosome 15 that codes for fibrillin 1, in the absence of which elastin is more readily degraded by matrix metalloproteinases and smooth muscle cells will dissociate from the medial matrix components.1,4
Pathophysiology and Follow-up
Aortic dilation is the most common cause of morbidity and mortality in patients with Marfan syndrome as dilation of the sinus of Valsalva is found in 60% to 80% of adult patients (Fig. 40-2).13 The relative abundance of elastic fibers in the ascending aorta compared with other regions of the arterial tree, coupled with the repetitive stress of LV ejection, probably accounts for aortic dilation that usually occurs primarily in the aortic root.13 Therefore, the majority of patients with Marfan syndrome present with enlargement of the ascending aorta or a type A dissection and only in very rare cases with a type B dissection involving the descending aorta.11 Aortic dissection is associated with increasing aortic diameter but it may also occur in nondilated aortas.11,12 Replacement of the aortic root with a composite graft conduit has been recommended before the diameter exceeds 5.0 to 5.5 cm.11,12 Independent predictors of progressive aortic dilation that will prompt the recommendation for surgery when the aorta is smaller than 5.0 cm include rapid growth of the aortic diameter (>1 cm/yr), family history of premature aortic dissection (<5 cm), greater than mild aortic regurgitation, and pregnancy or contemplated pregnancy.11,12 Aortic regurgitation may result from distortion of the coaptation of the aortic valve cusps by the enlarged aortic root and occurs in 15% to 44% of patients.11 Especially in young children, progression of findings is more important than absolute size of the aorta as a criterion for surgery.11
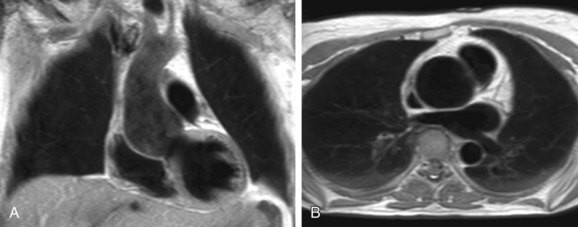
 FIGURE 40-2
FIGURE 40-2Recent MRI reports indicate that reduced aortic distensibility is an independent predictor of progressive aortic dilation in addition to aortic diameters.12 Because elastin fragmentation in the aortic media is scattered in an irregular pattern along the aorta, regional distensibility may be sensitive in the detection of regional variations in aortic stiffness.12 For optimal risk stratification, aortic stiffness may be taken into account in combination with aortic dimensions and the previously mentioned predictors of progressive aortic dilation.4,12,13 MRI has been recommended for routine assessment of aortic diameters and stiffness in patients with Marfan syndrome as well as for the follow-up of aortic complications, such as intramural hematoma and aortic aneurysms.4,11,12 Evaluation of aortic dilation should be performed every 6 months to determine the rate of progression, which can be extended to annual evaluation when the aortic size is stable over time.11 MRI can also be used to adequately monitor the beneficial effect of administration of β blockers on the progression rate of aortic dilation and reduction of aortic complications.11
BICUSPID AORTIC VALVE DISEASE
Prevalence and Epidemiology
The bicuspid aortic valve (BAV) is the most common congenital cardiac malformation, occurring in 1% to 2% of the population.14–16 BAV is the result of abnormal aortic cusp formation due to inadequate production of fibrillin 1 during valvulogenesis.2,4 Adjacent cusps fuse to form a single aberrant cusp, larger than its counterpart yet smaller than two normal cusps combined.2 BAV is probably the result of a complex developmental pathologic process rather than simply the fusion of two normal cusps.2,14,16
Pathophysiology and Follow-up
Aortic regurgitation is the most frequent (80%) complication in patients with BAV and usually occurs from cusp prolapse, fibrotic retraction, or dilation of the sinotubular junction, in many cases requiring aortic valve replacement.2,4 BAV is also present in the majority of elderly patients with significant aortic stenosis, reflecting the propensity for premature fibrosis, stiffening, and calcium deposition in these abnormally functioning valves.2,4 The vascular complications of BAV are less well understood and are associated with significant morbidity and mortality.2,16 The histology of the ascending aortic wall in patients with BAV shows strong similarities with the fibrillin 1–deficient aortas of patients with Marfan syndrome, with accelerated degeneration of the aortic media due to loss of fibrillin 1 microfibrils as well as focal abnormalities within the aortic media, such as matrix disruption and smooth muscle cell loss (see Fig. 40-1).1,14 Interestingly, BAV is present in more than 70% of patients with coarctation, and both conditions are by themselves and certainly in combination known to be associated with similar aortic wall abnormalities and concomitant aortic dilation.1,14
As a consequence of abnormal aortic wall composition in BAV, serious complications such as progressive aortic root dilation (50% to 60% of all patients with BAV; Fig. 40-3) and aneurysm formation may finally result in aortic dissection (5% of all patients with BAV).16,17 Despite this lower incidence of aortic dissection than in Marfan syndrome (40%), BAV is the more common etiology in aortic dissection because Marfan syndrome is a much rarer entity (0.01% vs. 1% to 2% of patients with BAV).2 Two different phenotypes of aortic dilation have been described. Dilation of the mid ascending aorta is most commonly present (70%) and is associated with aortic valve stenosis, suggesting a post-stenotic causative mechanism.16 Aortic root dilation is much rarer (13%), being determined by male gender and degree of aortic regurgitation.16 Aortic root replacement is generally more aggressively recommended for patients with BAV (i.e., 4 to 5 cm) than for those patients with a tricuspid aortic valve (i.e., 5 to 6 cm).2 Subdivision into the two existing phenotypes may further refine the surgical approach by suggesting aortic root sparing when only dilation of the mid ascending aorta is present.16
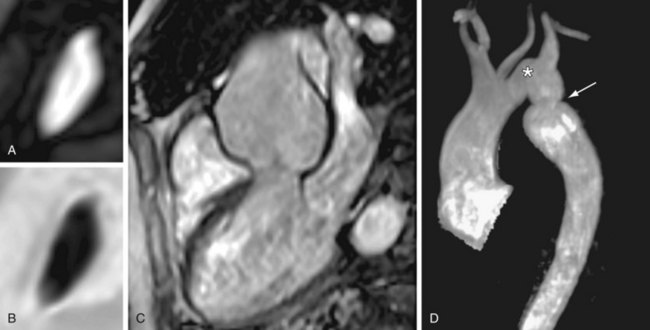
 FIGURE 40-3
FIGURE 40-3An MRI study reported frequent aortic root dilation and reduced elasticity in the entire aorta, suggesting not only that the proximal part of the aorta is affected in BAV but also that aortic wall lesions extend into the entire aorta.18 Evaluation of the elastic properties of the ascending aorta might be useful to identify patients who are at risk of progressive aortic dilation, analogous to patients with Marfan syndrome.12,18 Increased aortic stiffness was also associated with LV hypertrophy as a result of increased LV afterload.18 Sustained LV hypertrophy is associated with reduced diastolic filling; therefore, as diastolic LV dysfunction is a major contributor to congestive heart failure, LV hypertrophy might pose a future risk for LV function in patients with BAV.18 As many patients with BAV will require cardiac surgery during their lifetime, close monitoring of aortic dimensions, aortic elasticity, aortic valve competence, and LV function is mandatory during follow-up to allow timely intervention.18
COARCTATION OF THE AORTA
Prevalence and Epidemiology
Coarctation of the aorta accounts for 5% of all CHD and is defined as a congenital narrowing of the aorta, most commonly in a juxtaductal position just distal to the origin of the left subclavian artery.19 A wide spectrum of narrowing of the aorta can be observed, from a discrete narrowing to a hypoplastic aortic arch, whether or not it is associated with an intracardiac defect such as a ventricular septal defect or aortic valve disease.19 Classic symptoms are heart failure and an increased blood pressure proximal to the narrowing as well as a low perfusion status of the body distal to the coarctation.19 Coarctation of the aorta is associated with a significantly increased cardiovascular morbidity and reduced life expectancy even after successful surgical correction at a young age.7,12,20–22 Structural aortic wall abnormalities with reduced aortic elastic properties proximal and distal to the site of coarctation imply that coarctation of the aorta is a systemic vascular disease.4,20
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


