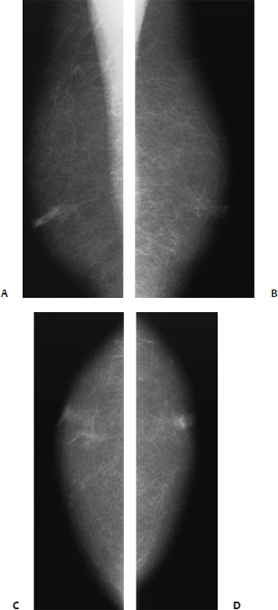
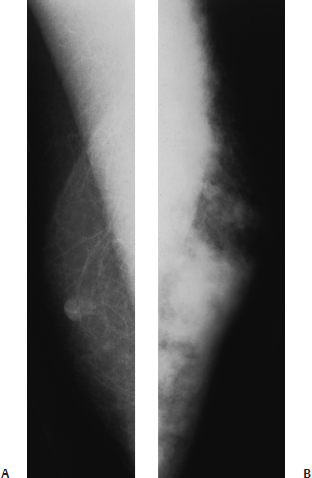
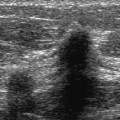
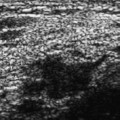
25 Malignant Male Breast A 77-year-old man presents with right bloody nipple discharge. • Right breast: bloody discharge easily expressed from nipple at the 2 o’clock position; normal nipple and areola • Left breast: normal exam Fig. 25.1 There is mild prominence of a right subareolar duct. The left breast is normal. (A) Right MLO mammogram. (B) Left MLO mammogram. (C) Right CC mammogram. (D) Left CC mammogram. • Ductal carcinoma in situ • BI-RADS assessment category 0; need additional imaging • Male breast cancer consists of less than 1% of all new breast cancer cases and only 0.2% of all newly discovered cancers in men. Infiltrating ductal carcinoma is the most common histology (approximately 85% of cases). Ductal carcinoma in situ comprises 5% of male breast cancers. Men develop ductal carcinoma in situ and invasive cancer later than women. Mean age at presentation is in the mid-60s. These tumors generally present with a nontender palpable mass. Nipple discharge is relatively common and is present in approximately 35% of patients with ductal carcinoma in situ and in 10 to 20% of those with invasive tumors. Other associated findings include skin thickening, nipple retraction, and axillary adenopathy. • Mammographically, invasive malignancies have a wide variety of appearances. They may be either well or ill defined. Their shapes include round, oval, lobulated, and irregular. Microcalcifications are present in 25 to 30% of tumors. Commonly, these calcifications are coarser than the ones found in female breast cancer. • Sonographically, male invasive malignancies have the same appearances as female tumors. However, male ductal carcinoma in situ differs from female ductal carcinoma in situ. The papillary subtype predominates in men, so male ductal carcinoma in situ lesions sonographically commonly appear associated with fluid collections or ducts. • Bloody discharge, a prominent duct, and no palpable mass suggest that ductography may be useful to identify the intraductal abnormality. Sonography may also be used to identify a focally dilated ductal system and guide intraoperative excision. However, this patient had no further imaging. The patient’s ducts were initially surgically excised. When ductal carcinoma in situ was identified, a mastectomy was performed. American Cancer Society. Cancer Facts and Figures: 2001. Atlanta: ACS; 2001 Appelbaum AH, Evans GFF, Levy KR, Amirkhan RH, Schumpert TD, Schumpert TD. Mammographic appearances of male breast disease. Radiographics 1999;19:559–568 Camus MG, Joshi MG, Mackarem G, et al. Ductal carcinoma in situ of the male breast. Cancer 1994;74:1289–1293 Hittmair AP, Lininger RA, Tavassoli FA. Ductal carcinoma in situ (DCIS) in the male breast: a morphologic study of 84 cases of pure DCIS and 30 cases of DCIS associated with invasive carcinoma—a preliminary report. Cancer 1998;83:2139–2149 Quimet-Oliva D, Hebert G, Ladouceur J. Radiographic characteristics of male breast cancer. Radiology 1978;129:37–40 Scott-Conner CEH, Jochimsen PR, Menck HR, Winchester DJ. An analysis of male and female breast cancer treatment and survival among demographically identical pairs of patients. Surgery 1999;126:775–780, discussion 780–781 A 68-year-old man presents with left breast swelling and shortness of breath. • Left breast: entire breast is hard and lumpy; diffuse skin thickening and erythema are present; palpable nodes are present in the left axillary and supraclavicular areas. • Right breast: normal exam • Chest: decreased breath sounds bilaterally at bases Mass (Fig. 25.2) • Margin: indistinct • Shape: irregular • Density: high density • Skin thickening • Trabecular thickening Fig. 25.2 The left breast shows marked, diffuse increase in density compared with the right breast. There is associated skin thickening and diffuse nodularity throughout the left breast. (A) Right MLO mammogram. (B) Left MLO mammogram.
Case 25.1: Ductal Carcinoma in Situ
Case History
Mammogram (Fig. 25.1)
Physical Examination
Pathology
Management
Pearls and Pitfalls
Suggested Reading
Case 25.2: Inflammatory Carcinoma
Case History
Physical Examination
Mammogram
Other Modalities: Chest Radiography and Bone Scan (Figs. 25.3 and 25.4)
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


