Mandible
The mandible is divided into the body anteriorly and the ramus posteriorly, with the angle of the mandible interposed between. The ramus ascends dividing into the coronoid process anteriorly and the condyle with its neck and head posteriorly. The masseter muscle inserts on the outer surface of the ramus and the medial pterygoid on the inner surface. The temporalis muscle inserts anteriorly on the coronoid process. The lateral pterygoid muscle inserts anteriorly on the neck of the condyle. There are 20 deciduous teeth: 2 incisors, 1 canine, and 2 molars in each quadrant. There are 32 permanent teeth: 2 incisors, 1 canine, 2 premolars, and 3 molars in each quadrant.
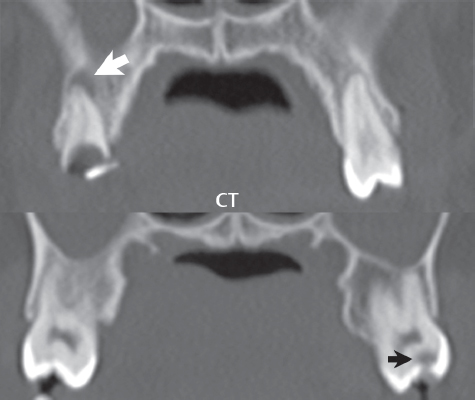
A Panorex is the standard plain film exam, for screening, of the mandible. It provides a survey (panoramic view) of the entire mandible and maxilla on a single image. CT provides excellent bony detail regarding the mandible, and a Panorex – like image can also be reconstructed. Dental caries are commonly incidentally visualized on CT, whether performed for trauma involving the face or inflammatory disease involving the paranasal sinuses ( Fig. 2.77 ). In regard to neoplastic disease, MR provides excellent assessment of extraosseous lesion extent, and is very sensitive to tumor invasion (of the mandible). Abnormalities involving the marrow of the mandible can be assessed on MR by the use of fat suppressed T2-weighted scans, T1-weighted scans (with obliteration of the normal high signal intensity fatty marrow implying tumor invasion), and fat suppressed T1-weighted postcontrast imaging.
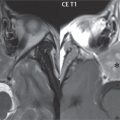
Osteonecrosis of the jaw (with that of the mandible most common) may be associated with osteomyelitis (due to dental infections), osteoradionecrosis in patients with prior radiation, metastatic disease, or with bisphosphonate use (bisphosphonate-related osteonecrosis of the jaw [BPONJ]). Patients with BPONJ typically present with tooth loosening and nonhealing extraction sockets. Bisphosphonates inhibit osteoclast-mediated bone resorption and are standard treatment for skeletal-related manifestations of multiple myeloma, breast carcinoma, and other solid cancers. CT demonstrates mixed sclerotic and lytic changes and occasionally pathologic fractures ( Fig. 2.78 ). MR typically manifests low T1 and high T2 signal intensity, with lesion enhancement. BPONJ is fluorodeoxyglucose (FDG) avid.

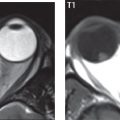
Dental cysts can be either odontogenic (associated with tooth development) or nonodontogenic. Radicular cysts (a.k.a. periodontal cysts) are the most common odontogenic cysts ( Fig. 2.79 ) and occur with untreated dental caries. Dentigerous (follicular) cysts are the next most common odontogenic cyst. They are unilocular and surround the crown of an unerupted tooth ( Fig. 2.80 ).

Fissural cysts are the most frequently encountered nonodontogenic cysts, the most common being the nasopalatine duct cyst (incisive canal cyst), with some cysts attaining sizes of 2 to 3 cm. The normal canal should measure approximately 6 mm and canals larger than this should be regarded with suspicion. Fissural cysts are most commonly encountered in the fourth to sixth decades with surgical enucleation the treatment of choice. Keratocystic odontogenic tumors are characterized by local aggressiveness and infiltration into surrounding tissues with a high rate of recurrence. They appear as an expansile multi- or unilocular cyst (not associated with a crown or unerupted tooth) with undulating borders, cortical thinning, and root resorption often occurring near the third molar tooth. They can be associated with Marfan and Noonan syndromes. When multiple, 50% are associated with nevoid basal cell carcinoma (Gorlin) syndrome.
An ameloblastoma is a benign, locally invasive neoplasm of odontogenic origin. Although it can involve either the mandible or maxilla, most are mandibular (80%). They occur in the third and fourth decades of life, and are slow growing and painless. On imaging ameloblastomas are usually bubbly multiloculated lesions (80%) often with extensive bony destruction ( Fig. 2.81 ). Ameloblastomas have a tendency to break through the cortex with formation of a soft tissue mass.

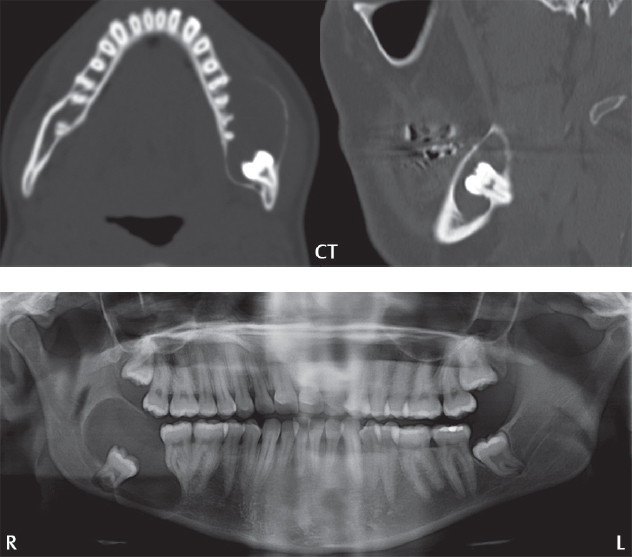
The mandible is commonly injured in trauma, due to its prominent position and ring-like configuration. Motor vehicle accidents and assaults are the primary causes of injury, and specifically fracture. A Panorex exam can miss subtle nondisplaced fractures, with CT advocated for optimal evaluation ( Fig. 2.82 ). Fractures involving the body may traverse the inferior alveolar canal, which runs from the mandibular foramen to the mental foramen, and can impair function of the inferior alveolar nerve (a branch of the mandibular [CN V3] nerve) resulting in lip/chin numbness. Due to its ring-like configuration, 50% of mandibular fractures are multiple (usually two breaks) ( Fig. 2.83 ) such as a parasymphyseal fracture and associated contralateral subcondylar fracture.


Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


