After studying this chapter, the student will be able to:
1. Assess the basic levels of neurologic and cognitive functioning.
2. List the three classifications of shock and describe the shock continuum.
3. Define distributive shock and the three different types.
4. Explain the role of the radiographer in recognizing and responding to the patient’s immediate medical needs in the various categories of shock.
5. List the clinical manifestations of pulmonary embolus and describe what the technologist’s response should be.
6. Differentiate among hypoglycemia, ketoacidosis, and hyperosmolar nonketotic syndrome, and explain the actions to be taken in response to these symptoms.
7. List the clinical manifestations of a cerebral vascular accident and explain the actions to be taken in response to these symptoms.
8. List the clinical manifestations of cardiac and respiratory failure and explain the actions to be taken in response to these symptoms.
9. Explain the symptoms of mechanical airway obstruction and the emergency intervention necessary if this is suspected.
10. Describe the actions to be taken if a patient were to faint or have a seizure while under the technologist’s care.
11. Describe the best way to assist an agitated or a confused patient and the intoxicated patient.
KEY TERMS
Anaphylaxis: The result of an exaggerated hypersensitivity reaction; an allergic reaction
Bradycardia: An abnormal circulatory condition in which the heart beats in a regular pattern but at a rate of less than 60 beats per minute
Bronchospasm: Contraction of smooth muscles in the walls of the bronchi and bronchioles, causing narrowing of the lumen
Diaphoresis: Profuse sweating, heavy perspiration
Periorbital: Relating to the periosteum of the orbit, usually of the eye
Polydipsia: Increased thirst
Polyphagia: Increased hunger
Polyuria: Increased urination
Psychosis: A state in which a person’s mental capacity to recognize reality, communicate, and relate to others is impaired
SOB: Shortness of breath; some may prefer the term “SOA” (shortness of air), but SOA also means “seen on arrival,” “stimulus onset activity,” and several other medical terms
Syncope: Fainting
Tachycardia: An abnormal condition in which the myocardium contracts at a rate greater than 100 beats per minute
Many patients come to the diagnostic imaging department in poor physical condition. This may be due to illness, injury, or a lengthy preparation for a diagnostic examination. When a person is in a weakened physical condition, physiologic reactions may not be as expected. Many abnormal physiologic reactions occur quickly and without warning and may be life threatening if not recognized and treated immediately. The nontrauma-related medical emergencies that are most likely to occur while the patient is undergoing diagnostic imaging are shock, anaphylaxis (a type of shock), pulmonary embolus, reactions related to diabetes mellitus, cerebral vascular accident (CVA), cardiac and respiratory failure, syncope, and seizures. As the first member of the health care team to observe these reactions, the radiographer must be able to recognize the symptoms and initiate the correct treatment.
The technologist must be able to assess the behaviors that determine a patient’s level of neurologic and cognitive functioning on admission for a diagnostic procedure. If this initial assessment is performed, the technologist will be able to recognize changes in the patient’s mental status if they occur while in the imaging department.
In most cases, the first action that should be taken in a life-threatening emergency is to call the hospital emergency team, the physician conducting the procedure, and a coworker for assistance. Every technologist must learn the correct procedure for calling the hospital emergency team in the institution of employment. In many health care institutions, this procedure is dubbed “calling a code” or CODE BLUE. Memorize the emergency team number, and be prepared to explain the exact location of the emergency and the problem that has occurred.
All imaging departments have an emergency cart that contains the medications and equipment that are needed when a patient’s condition suddenly becomes critical. This is often called the “crash cart.” Know where to obtain this cart quickly, and know who is responsible for maintaining the cart and having all its equipment and supplies in working order. Be familiar with the oxygen administration equipment so that assistance can be provided quickly.
DISPLAY 9-1 Glasgow Coma Scale
Eyes Open
Extension
2
Spontaneously
14
No response
1
To voice
3
Verbal Response
To painful stimuli
2
Oriented
5
No response
1
Confused speech
4
Motor Response
Inappropriate words
3
Obeys commands
6
Incomprehensible sounds
2
Localized pain
5
None
1
Withdraws from painful stimuli
4
Abnormal flexion
3
Total points possible
15
Although imaging technologists are not the health care workers who are responsible for a patient’s pain management during the majority of medical care, the technologist must be sensitive to complaints of pain and discomfort while the patient is in the imaging department.
ASSESSMENT OF NEUROLOGIC AND COGNITIVE FUNCTIONING
The technologist must be able to quickly assess the patient’s neurologic functioning, because if the patient’s condition deteriorates, it can be quickly recognized on the basis of changes in the initial assessment data. Neurologic assessment can be highly technical and complex and is not within the scope of a technologist’s practice. However, a rapid neurologic assessment tool that is used frequently in health care institutions is the Glasgow Coma Scale. This scale addresses the three areas of neurologic functioning and quickly gives an overview of the patient’s level of responsiveness. It is simple, reliable, and convenient to use.
Three areas can be readily observed—eyes opening, motor response, and verbal response. A patient can be rated a maximum of 15 points for neurologic functioning. If the patient’s score begins to drop after the initial assessment, notify the physician in charge of the patient immediately (Display 9-1).
Another indicator that a patient’s condition is deteriorating is a change in the level of consciousness (LOC). These changes can be subtle but must not be ignored. The LOC can be assessed quickly with the following three parameters:
1. Ask the patient to state certain items, such as name, date, address, and the reason for coming to the imaging department. If the patient gives these responses readily and correctly, then it can be assumed that the patient is responding to verbal stimuli and is oriented to person, place, time, and situation. Note any undue need to repeat questions and any slow response, difficulty with choice of words, or unusual irritability.
2. Note the patient’s ability to follow directions during instruction regarding positioning for the examination. Also note any movement that causes pain or other difficulty in movement, as well as any alterations in behavior or a lack of response. Report these to the physician in charge of caring for the patient. These measures provide a baseline against which changes in the patient’s mental and neurologic status can be assessed.
3. Assess the patient’s vital signs at this time if current readings are not on the chart. Chapter 6 describes how to perform baseline vital signs and the normal ranges. Baseline readings are a must to have in order to note any changes that may occur. An increasing systolic blood pressure or widening of the pulse pressure may indicate increasing intracranial pressure. Slowing of the pulse may also indicate increasing intracranial pressure. As compression of the brain increases, the vital signs change. Respirations increase, blood pressure decreases, and the pulse rate decreases further. A rapid rise in body temperature or a decrease in body temperature is also an ominous sign.
If the patient has no complaints on initial assessment, note this. If the patient begins to complain of a headache, becomes restless or unusually quiet, or develops slurred speech or a change in the level of orientation as a procedure progresses, report this to the physician immediately, stop the procedure, stay with the patient, and summon assistance. This includes requesting the emergency cart to be brought to the patient. Then, prepare the patient for oxygen and intravenous fluid administration.
WARNING!
Changes in a patient’s neurologic status or LOC must never be ignored! Stop work and notify the physician of these changes.
SHOCK
Shock is the body’s pathologic reaction to illness, trauma, or severe physiologic or emotional stress. It may be caused by body fluid loss, cardiac failure, decreased tone of the blood vessels, or obstruction of blood flow to the vital body organs. Shock causes the body to suffer from insufficient blood flow to the body. It is a life-threatening condition that may occur rapidly and without warning. It may be reversible if it is not allowed to progress. The technologist may be the first health care worker to observe the initial symptoms of shock; therefore, it is important to recognize them and begin the interventions that will halt its progress, which will eventually lead to organ failure and death.
The Shock Continuum
The vital organs of the body depend on oxygen and other nutrients supplied by the blood for their survival. When this supply is diminished, adverse effects on normal physiologic functions occur. The shock syndrome may progress as a continuum in the patient’s struggle to survive and return to a normal physiologic state.
At the onset of the shock continuum, the changes in physiologic function are in the cells of the body and are not clinically detectable except for a possible increase in heart rate. As the condition progresses, blood is shunted away from the lungs, skin, kidneys, and gastrointestinal tract to accommodate the brain’s and the heart’s critical need for oxygen. At this stage, called the compensatory stage, a host of symptoms is noticeable:
1. Cold and clammy skin
2. Nausea and dizziness
3. Increased respirations (shortness of breath [SOB])
4. Anxiety level increases; patient may begin to be uncooperative
5. Blood pressure is decreased, and pulse rate is increased
If shock is allowed to progress beyond the compensatory stage, the mean arterial pressure (the average pressure at which the blood moves through the vasculature of the body) falls. All body systems are inadequately perfused, including the heart, which begins to pump inadequately. Vasoconstriction reduces arterial blood flow into organs and their tissues, causing ischemia and necrosis.
The peripheral circulation reacts to the chemical mediators released by the body in this state, and fluid leaks from the capillaries, further decreasing the amount of fluid in circulation. The patient has acute renal failure, and the liver, gastrointestinal, and hematologic systems begin to fail. This stage in the shock continuum is called the progressive stage. Progressive stage symptoms include:
1. Significantly decreased blood pressure with an increase in pulse rate.
2. Respirations are rapid and shallow.
3. Pulmonary capillaries leak fluid into the lungs, causing severe pulmonary edema, known as acute respiratory distress or shock lung.
4. Tachycardia results and may be as rapid as 150 beats per minute.
5. Chest pain may occur.
6. Mental status begins to change with subtle behavior alterations such as confusion with progression to lethargy and loss of consciousness.
7. Renal, hepatic, gastrointestinal, and hematologic problems occur.
If shock progresses beyond this point, it is called the irreversible stage. The organ systems of the body suffer irreparable damage, and recovery is unlikely.
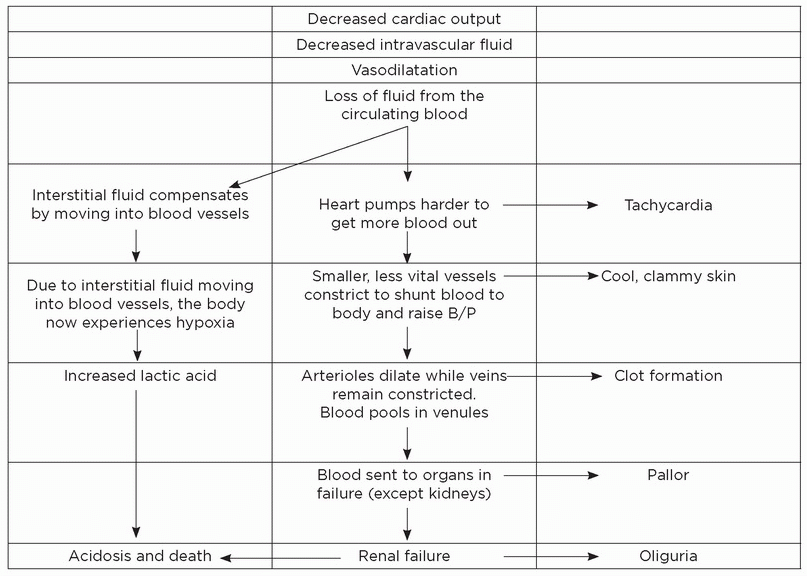
DISPLAY 9-2 Progression of Shock with Associated Symptoms
Irreversible stage involves the following:
1. Low blood pressure.
2. Renal and liver failure.
3. Release of necrotic tissue toxins and overwhelming lactic acidosis.
Display 9-2 shows the progression of shock with the corresponding symptoms. There are different classifications of shock. These include hypovolemic, cardiogenic, and distributive or obstructive shock. The following sections provide descriptions, clinical manifestations, and the technologist’s response to each of these.
Hypovolemic Shock
Body fluids are contained within the cells of the body and are in the extracellular compartments. The extracellular fluid is further distributed to the blood vessels (intravascular) and into the surrounding body tissues (interstitial). Approximately three or four times more body fluid is within the interstitial spaces than within the vasculature of the body. When the amount of intravascular fluid decreases by 15% to 25% or by a loss of 750 to 1,300 mL, hypovolemic shock occurs. This decrease in volume may be due to internal or external hemorrhage; loss of plasma from burns; or fluid loss from prolonged vomiting, diarrhea, or medications.
Clinical Manifestations
The signs and symptoms of hypovolemic shock may be placed into the following classes:
Class I: A blood loss of 15%
Blood pressure is within normal limits.
Heart rate is less than 100 beats per minute.
Respiration ranges from 14 to 20 per minute.
Class II: A blood loss of 15% to 30%
Blood pressure is within normal limits.
Heart rate is greater than 100 beats per minute.
Respiration ranges from 20 to 30 per minute.
Class III: A blood loss of 30% to 40%
Blood pressure begins to decrease to below normal limits.
Heart rate is greater than 120 beats per minute.
Respiration increases to 30 to 40 per minute.
Class IV: A blood loss of 40% or more
Systolic blood pressure decreases from 90 to 60 mm Hg.
Heart rate is now in tachycardia with a weak and thready pulse.
Respiration is greater than 40 per minute.
The patient may become excessively thirsty as a result of the fluid loss from hypovolemic shock. The extremities are cold; the skin is cold and clammy with cyanosis starting at the lips and nails. If the patient is dark-skinned, cyanosis may be observed by pressing lightly on the fingernails or earlobes. If the patient is cyanotic, the color will not return to the compressed area in the usual 1-second interval. A bluish discoloration of the tongue and soft palate of the mouth is also indicative of cyanosis. If this condition is allowed to continue, cardiac and respiratory failure follows.
Response
1. Stop the ongoing procedure; place the patient supine with legs elevated 30° (if there is no head or spinal cord injury). Do not place the patient in the Trendelenburg position.
2. Notify the physician in charge and call for emergency assistance from the department nurse.
3. Make certain that the patient is able to breathe without obstruction caused by position or blood or mucus in the airway.
4. If there is an open wound with blood loss, put on clean gloves and apply pressure directly to the wound with several thicknesses of dry, sterile dressing.
5. Bring the emergency cart to the room.
6. Prepare to assist with oxygen, intravenous fluids, and medications.
7. Keep the patient warm and dry, but do not overheat the patient because this will increase the need for oxygen.
8. Assess vital signs every 5 minutes until the emergency team assumes this role.
9. Do not leave the patient unattended. If there is anxiety, explain what is happening.
10. Do not offer fluids to the patient, even if requested. Explain that any subsequent examination or treatment that may require an empty stomach.
Cardiogenic Shock
Cardiogenic shock is caused by a failure of the heart to pump an adequate amount of blood to the vital organs. The onset of cardiogenic shock may occur over a period, or it may be sudden. The patient who has been hospitalized for myocardial infarction, dysrhythmias, or other cardiac pathology is most vulnerable. A subcategory, obstructive shock, is caused by a cardiac tamponade, a pulmonary embolus, pulmonary hypertension, arterial stenosis, constrictive pericarditis, or tumors that are blocking blood flow through the heart.
Clinical Manifestations
Complaint of chest pain that may radiate to jaws and arms
Dizziness and respiratory distress
Cyanosis
Restlessness and anxiety
Rapid change in the LOC
Pulse may be irregular and slow; may have tachycardia and tachypnea
Difficult-to-find carotid pulse indicates decreased stroke volume of the heart
Decreasing blood pressure
Decreasing urinary output
Cool, clammy skin
Response
1. Summon the emergency team and have the emergency cart placed at the patient’s side.
2. Notify the physician in charge of the patient.
3. Place the patient in the semi-Fowler position or in another position that will facilitate respiration.
4. Prepare to assist with oxygen, intravenous fluid, and medication administration. Chest pain must be controlled.
5. Do not leave the patient alone; offer an explanation of treatment as appropriate; alleviate the patient’s anxiety.
6. Assess pulse, respiration, and blood pressure every 5 minutes until the emergency team arrives.
7. Do not offer fluids.
8. Be prepared to administer cardiopulmonary resuscitation (CPR), if indicated
Distributive Shock
Distributive shock occurs when a pooling of blood in the peripheral blood vessels results in decreased venous return of blood to the heart, decreased blood pressure, and decreased tissue perfusion. This may be the result of loss of sympathetic tone. Distributive shock is characterized by the blood vessels’ inability to constrict and their resultant inability to assist in the return of the blood to the heart. It may also occur when chemicals released by the cells cause vasodilatation and capillary permeability, which in turn prompts a large portion of the blood volume to pool peripherally. There are three types of distributive shock: neurogenic, septic, and anaphylactic.
Neurogenic Shock
Neurogenic shock results from loss of sympathetic tone, causing vasodilatation of peripheral vessels. Spinal cord injury, severe pain, neurologic damage, the depressant action of medication, a lack of glucose (as in insulin reaction or shock), or the adverse effects of anesthesia can all cause neurogenic shock.
Clinical Manifestations
Hypotension
Bradycardia
Warm, dry skin
Initial alertness if not unconscious because of head injursy
Cool extremities and diminishing peripheral pulses
Response
1. Summon emergency assistance.
2. Notify the physician in charge of the patient.
3. Keep the patient in a supine position; legs may be elevated with physician’s orders.
4. Have the emergency cart brought to the patient’s side.
5. If spinal cord injury is possible, do not move the patient.
6. Stay with the patient and offer support.
7. Monitor pulse, respirations, and blood pressure every 5 minutes.
8. Prepare to assist with oxygen, intravenous fluids, and medications.
Septic Shock
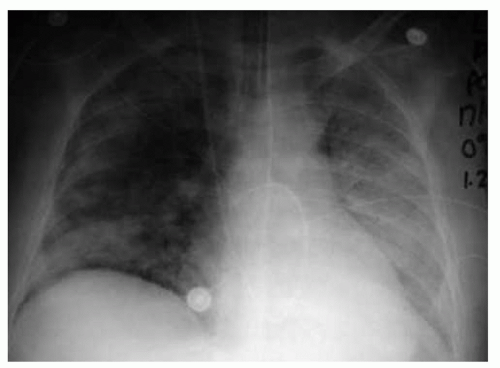
Septic shock is the least likely to be observed by the radiographer in the imaging department. However, radiographers must be able to recognize septic shock. Patients in the intensive care unit or emergency room who are in septic shock may need to have a mobile radiograph taken. Radiographic studies used to evaluate patients with suspected sepsis or septic shock include chest, abdomen, and extremity radiography. Chest radiography is most common because most patients with sepsis have pneumonia (Fig. 9-1).
Gram-negative bacteria are the most common causative organisms in septic shock; however, gram-positive bacteria and viruses can be the cause. When invaded by bacteria, the body begins its immune response by releasing chemicals that increase capillary permeability and vasodilatation, leading to the shock syndrome.
Clinical Manifestations
The clinical manifestations of septic shock are divided into two phases:
First Phase:
Hot, dry, and flushed skin
Increase in heart rate and respiratory rate
Fever, but possibly not in the elderly patient
Nausea, vomiting, and diarrhea
Normal to excessive urine output
Possible confusion, most commonly in the elderly patient
FIGURE 9-1 A 45-year-old woman was admitted to the intensive care unit with septic shock secondary to spontaneous biliary peritonitis.
Second Phase:
Cool, pale skin
Normal or subnormal temperature
Drop in blood pressure
Rapid heart rate and respiratory rate
Oliguria or anuria
Seizures and organ failure if syndrome is not reversed
Response
The technologist is rarely the person who initiates action if septic shock is present. However, if a patient in septic shock is in the imaging department, care must be taken to ensure that the patient does not become chilled, because shivering increases the body’s oxygen consumption.
Anaphylactic Shock
Because some imaging procedures use contrast media that contain iodine, to which some people are allergic, this is the most frequently seen type of shock in radiographic imaging. The radiographer must be able to recognize it at its onset to prevent life-threatening consequences.
Anaphylactic shock (anaphylaxis) is the result of an exaggerated hypersensitivity reaction (allergic reaction) to re-exposure to an antigen that was previously encountered by the body’s immune system. When this occurs, histamine and bradykinin are released, causing widespread vasodilatation, which results in peripheral pooling of blood. This response is accompanied by contraction of nonvascular smooth muscles, particularly the smooth muscles of the respiratory tract. This combined reaction produces shock, respiratory failure, and death within minutes after exposure to the allergen. Usually, the more abrupt the onset of anaphylaxis, the more severe the reaction will be.
The most common causes of anaphylaxis are medications, iodinated contrast media, and insect venoms. The path of entry may be through the skin, respiratory tract, or gastrointestinal tract or through injection.
The technologist performing the procedure in which contrast media are injected is responsible for the patient. A meticulous history of previous allergic responses that the patient may have had to any medication or food, including previous incidents when receiving contrast agents in imaging, must be obtained. If any of these responses are reported, the technologist must be informed before injection of any contrast media.
When iodinated contrast media are being used for diagnostic procedures, observe the patient continuously for signs of allergic reaction. If early symptoms of anaphylactic shock are observed, quick action must be taken to halt the progression of symptoms.
Clinical Manifestations
The signs of anaphylactic shock may be classified as mild, moderate, or severe as follows:
Mild Systemic Reaction:
Nasal congestion, periorbital swelling, itching, sneezing, and tearing of eyes
Peripheral tingling or itching at the site of injection
Feeling of fullness or tightness of the chest, mouth, or throat
Feeling of anxiety or nervousness
Moderate Systemic Reaction:
All the foregoing symptoms, plus the following:
Flushing, feeling of warmth, itching, and urticaria
Bronchospasm and edema of the airways or larynx
Dyspnea, cough, and wheezing
Severe Systemic Reaction:
All symptoms listed above with an abrupt onset
Decreasing blood pressure; weak, thready pulse either rapid or shallow
Rapid progression to bronchospasm, laryngeal edema, severe dyspnea, and cyanosis
Dysphasia, abdominal cramping, vomiting, and diarrhea
Seizures and respiratory and cardiac arrest
Response
1. Do not leave the patient. Stop any infusion or injection of contrast immediately and notify the radiologist or department physician if any of the symptoms occur.
2. If the patient complains of respiratory distress or has any of the symptoms listed in the severe reaction section, call the emergency team.
3. Place the patient in the semi-Fowler position or in a sitting position to facilitate respiration.
4. Monitor pulse, respiration, and blood pressure every 5 minutes or until the emergency team arrives to assume responsibility.
5. Prepare to assist with oxygen, intravenous fluid, and medication administration. Have large-gauge venous catheters available.
6. Prepare to administer CPR as required.
The medications usually given for anaphylactic shock are epinephrine, diphenhydramine, hydrocortisone, and aminophylline.
Many imaging departments have a standardized procedure form that must be completed before the administration of contrast media. This form may request the information shown in Display 9-3.
DISPLAY 9-3 Information Requested before Administration of Contrast Agents
Name
Blood urea nitrogen and creatinine
Age
Have you had any protein in your urine? If so, to what degree?
Date
Do you have heart disease?
Have you had the study you are having today at any other
time? Hypertension?
If the answer is yes, did you have any allergic or unusual reaction?
Diabetes mellitus?
Are you allergic to any food, medications, or any other substances? If you are, please specify.
Sickle cell anemia?
Recent laboratory tests performed and results
Asthma?
Have you had any procedures that involved use of contrast agents? If so, please explain.
After the examination, the physician completes a report indicating the type of contrast agent used and any unusual responses. If the patient has an anaphylactic reaction, the nature of the reaction should be written on the patient’s imaging history. The person performing the injection and examination must also make documentation of the reaction in the patient’s chart.
A copy of this report is kept in the patient’s diagnostic imaging department file, and the department supervisor also keeps a copy. If these precautions in documentation are taken, the history of the patient’s previous problem will be on record, and the correct decisions can be made subsequently.
Patients who have received contrast media as part of the diagnostic imaging procedure should remain in the department for 30 minutes for observation if they are not patients in the hospital. If they are having no problems after 30 minutes, they may be allowed to return home, accompanied by another person. They should be clearly instructed in the signs and symptoms of an anaphylactic reaction and told to return to the hospital emergency department (ED) immediately if any of these symptoms appear. A patient who has had even a mild allergic reaction during a diagnostic procedure that involves the use of a contrast medium should be instructed to report this if he or she is ever to receive iodinated contrast media in the future. If the reaction was severe, the patient may need to wear an alert bracelet to prevent further exposure to antigens of this sort. Chapter 15 details the pharmacology of contrast media in detail, and special attention should be paid to this because contrast reactions are unpredictable.
Only gold members can continue reading. Log In or Register to continue