CHAPTER 27 Meningioma
Epidemiology
Meningiomas represent up to 18% of all intracranial tumors, with 7% of intracranial meningiomas arising on the anterior or posterior walls of the temporal bone.
Middle ear meningiomas are rare tumors that essentially always represent intratemporal extension of more common intracranial meningiomas. Like meningiomas in general, they are most often seen in middle-aged women. True primary middle ear meningiomas are very rare and remain reportable.
Clinical Features
Most patients present with posterior fossa symptoms due to the bulk of the meningioma arising at the skull base with the temporal bone involvement representing secondary extension. However, a chronic history of conductive hearing loss, tinnitus, otalgia, facial nerve palsy, or chronic otitis has been reported as a presenting symptom in patients with meningioma involving the temporal bone. This is not entirely surprising, as meningiomas are usually slow-growing tumors that can become quite large within the intracranial compartment while remaining clinically silent.
Pathology
Temporal bone meningiomas are histologically similar to typical intracranial meningiomas. They are considered benign lesions.
True primary middle ear meningiomas, if they exist, probably arise from ectopic neural crest arachnoidal cells.
Treatment
Aggressive surgery to remove the temporal bone portion of the lesion is the treatment of choice, particularly when middle ear symptoms are present. No chemotherapy is necessary, as these lesions are benign. Radiation therapy is reserved for recurrent, nonoperable lesions.
Imaging Findings
Most of these lesions are associated with a larger posterior fossa component with imaging characteristics typical of meningioma. However, the extremely rare, purely intratemporal meningioma appears as a nonspecific benign-appearing, nonaggressive mass.
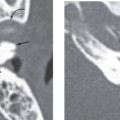
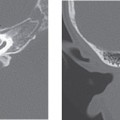
CT
Thin-section (1 to 2 mm) noncontrast computed tomography (CT) performed in the axial and coronal planes and reconstructed with a detail (bone) algorithm best delineate the temporal bone and its contents. Sagittal reformatted images are also sometimes useful. Small middle ear meningiomas, and ossicular or temporal bone erosion or sclerotic/permeative changes due to frank intraosseous invasion by meningioma (due to intratemporal extension by a contiguous posterior fossa meningioma) are best delineated on CT scans.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


