Miscellaneous Chest Diseases
ACUTE RESPIRATORY DISTRESS SYNDROME
Acute Respiratory Distress Syndrome
Background
Acute respiratory distress syndrome (ARDS) occurs when the pulmonary system is affected as a result of more generalized, multiorgan capillary damage.1 The pathogenic sequence appears related to inappropriate activation of the complement cascade,2,3 resulting in increased capillary permeability and pulmonary edema. Eventually fluid spills into the alveolar spaces, leading to hemorrhaging, reduced surfactant levels, and a resultant smaller functional area for gas exchange. A wide range of factors and conditions are associated with the development of ARDS (Box 26-1).
Imaging Findings
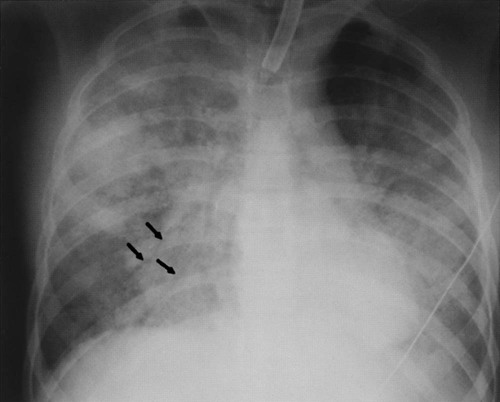
No changes are detectable radiographically during the initial stage of ARDS unless caused by pneumonia, aspiration, or another pulmonary condition, in which case the pulmonary findings of the concurrent disease may be noted. The latter stages of the disease are marked by alveolar filling. Patchy areas of incomplete lung consolidation are noted at first (Fig. 26-1), which eventually become more uniform, generalized, and homogenous. The radiographically detectable features gradually resolve during the ensuing weeks. Pleural effusion is rare.
Clinical Comments
ARDS is characterized by rapidly progressing respiratory distress.4,5 Alveolar filling is followed by acute respiratory failure requiring mechanical ventilation and oxygen administration. The eventual clinical outcome depends heavily on whether the patient develops a nosocomial infection, hemorrhage, sepsis, lung barotrauma, or another major complication.3
Extrinsic Allergic Alveolitis
Background
Extrinsic allergic alveolitis (EAA), also known as hypersensitivity pneumonitis, is a nonatopic, nonasthmatic allergic lung disease. EAA manifests as an occupational lung disease caused by the inhalation of organic dusts; this then produces granulomatous and interstitial lung changes. Table 26-1 lists several etiologic agents.
TABLE 26-1
SELECTED PROVOCATIVE AGENTS OF EXTRINSIC ALLERGIC ALVEOLITIS
| Disease | Provocative agent |
| Bagassosis | Moldy sugar cane |
| Bird fancier’s lung | Avian excreta |
| Farmer’s lung | Moldy hay |
| Humidifier lung | Contamination from humidifying, heating, and air conditioning systems |
| Malt worker’s lung | Moldy malt |
| Maple bark stripper’s lung | Moldy maple bark |
| Mushroom worker’s lung | Mushroom spores |
| Sequoiosis | Redwood dust |
| Suberosis | Moldy cork dust |
Imaging Findings
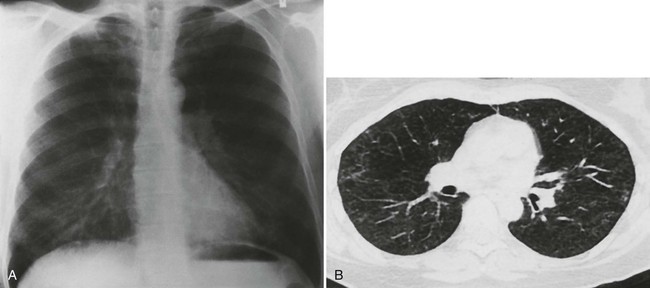
The radiographic presentation of EAA is the same regardless of the type of organic dust inhaled,6 but varies according to intensity of exposure.7 The early stages of EAA are characterized by reversible, multiple, small (1- to 3-mm), nodular radiodensities scattered bilaterally throughout the lung zones; although less common, the lung apices may be spared (Fig. 26-2).8–12 Repeated exposures may result in a chronic interstitial (honeycomb) pattern11 with upper lobe predominance.
Clinical Comments
Acute EAA is characterized by sudden onset of malaise, chills, fever, cough, dyspnea, and nausea within hours after exposure to the offending agent. Subacute and chronic forms are characterized by a persistent cough and slowly progressing dyspnea, anorexia, and weight loss. The patient’s history of exposure preceding the clinical symptoms is important for a proper diagnosis.
Pneumoconioses
Background
Pneumoconioses are a group of diseases caused by inhalation of inorganic dust and its accumulation in the lung.7 The dust deposits cause a nonneoplastic lung reaction that may be seen on radiographs. Asbestos, silicon, talc, beryllium, and coal dust incite a fibrogenic tissue reaction throughout the lung.13 Tin, barium, iron, and other inert particles do not incite fibrogenic changes but do cause particle-laden macrophages to accumulate in the lung.14 These reactions are called benign pneumoconioses (even though their radiographic appearance can be dramatic) because they are less aggressive.
Imaging Findings
The chest radiograph is the primary means of determining the presence and extent of pneumoconiosis.15 The International Labor Office (ILO) has established a classification system for the radiographic appearance of pneumoconioses16,17 that focuses on the size and shape of the lung nodules. The classification also includes a detailed categorization of pleural thickening.
The radiographic appearance of pneumoconiosis depends on the type and amount of dust inhaled and individual immunologic lung reactions (Table 26-2).18,19
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


