FIGURE 19.24 de Quervain’s disease. T2-weighted fat-suppressed coronal MR image (A) shows fluid distending the first extensor compartment (arrowheads) with synovial irregularity. Sequential T2*-weighted axial MR images from proximal (B) to distal (C) show abnormal morphology of the tendons with longitudinal splitting (arrowhead), distension of the compartment with fluid (arrow), and erosion of the adjacent radial styloid (curved arrow).
The MRI findings include those of tendinosis. The diagnosis of tendinosis is characterized by abnormal morphology in the form of thickening (can be determined by comparing with the relative size of the tendons in Compartments 2 through 6) or abnormal signal intensity characterized by increased signal intensity on T1-weighted images that does not brighten to the level of simple fluid on fluid-sensitive sequences. Tears of the tendons superimposed on tendinosis can also be encountered (Fig. 19.24). The presence of fluid localized to the tendon sheath or compartment as well as surrounding soft tissue edema with loss of adjacent fat planes and adjacent bone marrow edema at the radial styloid can also help to establish this diagnosis (Fig. 19.25). It has been reported in the literature that the isolated finding of increased signal intensity within the tendon substance is an unreliable sign of de Quervain’s disease (26, 27).
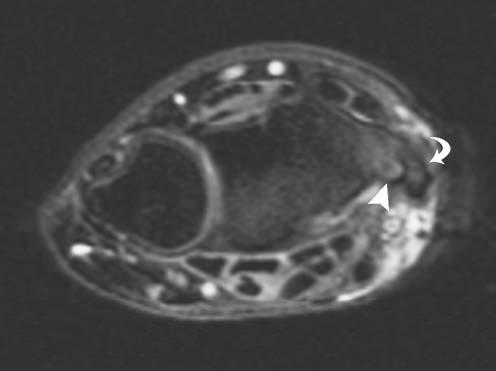
FIGURE 19.25 de Quervain’s disease. T2-weighted fat-suppressed axial MR image shows thickening of the tendons of the first extensor compartment (curved arrow) with bone marrow edema and erosive change (arrowhead) in the adjacent radial styloid.
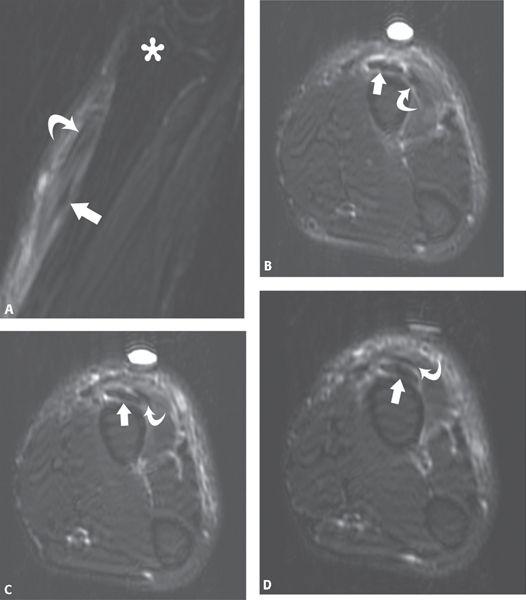
FIGURE 19.26 Intersection syndrome between the first and second extensor compartments. T2-weighted fat-suppressed sagittal (A) and sequential axial (B–D) MR images through the forearm show edema surrounding the ten-dons of the abductor pollicis longus and extensor pollicis brevis (curved arrow) as they cross over the extensor carpi radialis longus and brevis (straight arrow). The radial styloid (asterisk) is noted in the sagittal (A) image as a frame of reference.
This is a disease process that occurs more commonly in women and may be bilateral in up to 30% of patients. Chronic repetitive microtrauma from radial and ulnar deviation of the wrist has been considered a predisposing factor for this process (27–29). Associated structural variations that have been reported with this condition include the presence of a septum separating the first extensor tendon compartment tendons (27, 30). de Quervain’s disease has also been reported in association with the underlying conditions of myxedema, gout, and rheumatoid arthritis.
Intersection Syndrome
The intersection syndrome is an inflammatory process that affects the second extensor compartment tendons approximately 4 to 8 cm proximal to Lister’s tubercle at the junction of Zones VII and VIII (27, 31). A focal inflammation occurs at the point where the first extensor compartment tendons cross over the tendons of the second extensor compartment (Fig. 19.4). This type of process can also occur at the point where the third extensor compartment tendons cross over those of the second. This is most commonly the result of a friction syndrome from overuse and chronic repetitive microtrauma, previously associated with sports such as rowing, racket sports, and canoeing (32). Tendon sheath stenosis has also been identified as a causative factor (33).
The MRI findings that help to establish this diagnosis are those of peritendinitis. Fluid can be identified about the first and second compartment tendons and tendon sheaths. This occurs at the point where the compartments cross each other (Figs. 19.26 and 19.27). Tendinosis may be identified and adventitial bursa formation can also occur.
Traumatic Injuries
The classification of tendon injuries can be based on location using Verdan’s zone system previously described in this article (Fig. 19.1). In addition, injuries are often subdivided as open wounds resulting primarily from lacerations or closed wounds.
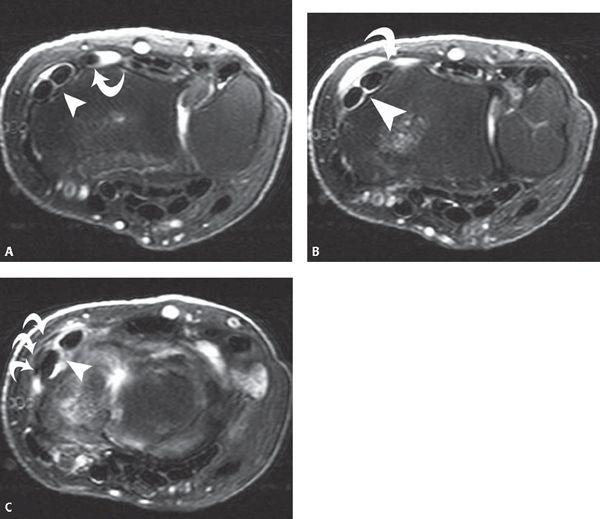
FIGURE 19.27 Intersection syndrome between the second and third extensor compartments. Sequential T2-weighted fat-suppressed axial MR images (A–C) from proximal to distal demonstrate fluid surrounding the extensor pollicis longus tendon (curved arrow) as it crosses over the extensor carpi radialis longus and brevis tendons (arrowhead). As the extensor pollicis longus crosses over the extensor carpi radialis longus and brevis (B), it becomes somewhat attenuated and flattened in configuration. After the crossover, there is a trilobed appearance to the extensor pollicis longus (curved arrows) (C) consistent with a partial tear.
Open Injuries
Open injuries are most often the result of lacerations and predominate at the levels of the middle phalanx (Zone II), the proximal phalanx (Zone IV), the MCP joint (Zone V), and the dorsum of the hand (Zone VI). The extensor tendons are particularly prone to injury from laceration as a result of their superficial location.
In the evaluation of any tendon injury, the integrity of the tendon must first be established. A combination of the sagittal and axial images serves this purpose best and allows the radiologist to identify focal areas of partial or complete discontinuity. The characterization of the margins of the tendon lesion, sharp and linear in the case of laceration, as well as the presence of an adjacent soft tissue defect can provide information to suggest the mechanism of injury in the absence of clinical history (Fig. 19.28). In any case of tendon rupture, the gap between the torn ends of the tendon should be described and precisely localized. The overall quality of the tendon (presence of underlying tendinosis) should be assessed. Any adjacent soft tissue or osseous abnormalities should be described.
At the level of the middle phalanx (Zone II), the conjoined tendons are thin and delicate. As a result of the radial and ulnar position of the tendons around the middle phalanx, a simple laceration rarely transects the entire extensor apparatus. If possible, the degree of tendon abnormality should be described as an injury involving less than 50% of the tendon width resulting in conservative treatment with routine wound care and splinting, whereas greater than 50% tendon width involvement necessitates primary repair (1, 34). More distally in this region in Zone I, the terminal tendon is well defined and dorsally positioned. Complete laceration of the terminal tendon will result in a flexed posture of approximately 40 degrees at the DIP joint. An incomplete laceration will result in a lesser extension lag of up to 15 degrees and a decrease in the strength of extension against resistance from a flexed position.
Although the dorsal apparatus is thin at this level, it is circumferentially oriented about the proximal phalanx and proximal IP joint. For this reason, simple injuries in Zones III and IV seldom result in complete laceration of the dorsal apparatus. The lacerated tendon ends do not retract appreciably as a result of their interconnections and because of the retinacular ligaments (1, 18). If the injury extends into Zone III, additional considerations include the possibility of extension into the PIP joint. If the capsule is violated, the joint must be thoroughly débrided, irrigated, and prophylactic antibiotics used. Injuries in Zone III also occur where the contribution of the extensors and lateral bands combine to form the central slip. Open injuries of the central slip may cause an acute boutonniere deformity.
Lesions at the MCP joint (Zone V) are almost always open and are commonly secondary to a human bite (Fig. 19.29). In simple lacerations at this level, the tendon ends do not retract. The injury often occurs in the clenched fist with the MCP in flexion. In this setting, the extensor tendon laceration is often proximal to the skin laceration as a result of the hand position when the injury is acquired. If an oblique laceration is present, the injury can be associated with injuries to the extensor hood, in particular the sagittal band, which can, in turn, lead to tendon subluxation or dislocation. Because of the possibility of open injuries of the MCP joint, the capsule must be closely scrutinized to ensure its integrity.
At the dorsum of the hand (Zone VI), the extensor tendons are very superficial. A trivial-appearing skin injury may result in the laceration of one or more ten-dons. Single or partial lacerations may not result in the loss of extension at the MCP joint on physical examination as a result of the duplication of tendons and the presence of intertendinous connections (1, 3). For this very reason, the imaging interpretation of tendon lesions can be challenging. In more complex injuries, injury to the paratenon or the underlying periosteum increases the risk of adhesions between the tendon and adjacent tissues. Tendon injuries at these levels are often associated with lacerations of branches of the superficial radial and dorsal ulnar nerves.

FIGURE 19.28 Laceration of the extensor tendon. T2*-weighted sagittal MR image through the finger shows the proximal (curved arrow) and distal (arrowhead) ends of the extensor tendon after a laceration. The sharp edges of the margins of the torn tendon ends suggest the mechanism of laceration.
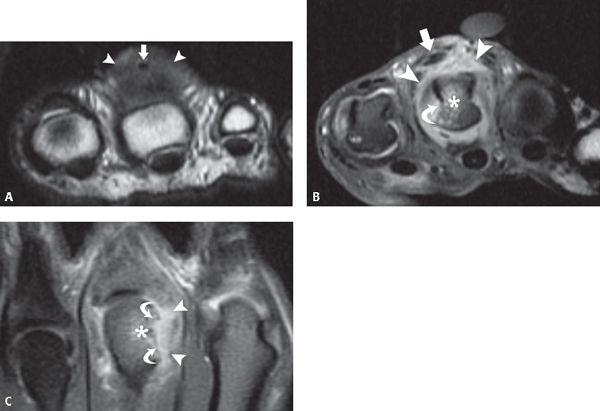
FIGURE 19.29 Septic arthritis after a human bite. T1-weighted axial MR image (A) shows dorsal soft tissue thickening (arrowheads) distal to the third metacarpophalangeal joint surrounding a low-signal–intensity focus (arrow) thought to represent a foreign body or gas. Corresponding T1-weighted fat-suppressed axial (B) and coronal (C) MR images after the administration of intravenous gadolinium show the sagittal band discontinuous from the ulnar side of the extensor tendon (arrow) with resultant radial displacement of the tendon. In addition, there is bone marrow edema (asterisk) in the metacarpal head and an erosion (curved arrow) consistent with septic arthritis and osteomyelitis. Enhancing synovitis surrounds the osseous structures of the articulation (arrowheads).
Closed Injuries
For anatomically related reasons, there are two types of closed extensor injuries that are of special interest in the fingers. The central slip and the terminal tendon insert into the dorsal osseous prominences of the middle and distal phalanges, respectively. Direct, deep contusions or joint injuries that result in acute instability may attenuate or avulse these tendons near their insertions. A terminal tendon injury may progress to a mallet deformity. Similarly, a central slip injury can progress to a boutonniere deformity. Because of the closed nature of the injuries, both diagnoses are often missed or undertreated. In addition to these injuries, extensor tendon subluxation or dislocation at the MCP can be encountered, primarily as a result of lesions of the sagittal bands.
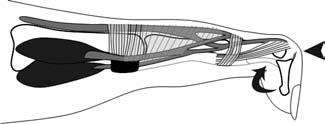
FIGURE 19.30 Diagram of the Mallet finger. In this injury, the extensor tendon is torn from its attachment to the dorsal aspect of the distal tuft of the finger (arrowhead). This results in unopposed action of the flexor tendon (curved arrow) and a flexion deformity at the distal interphalangeal.

FIGURE 19.31 Mallet finger. Lateral radiograph of the finger shows an avulsion of the osseous attachment of the extensor tendon from the dorsal aspect of the base of the distal phalanx of the finger. There is minimal displacement of the avulsed fragment. The alignment pattern appears neutral as a result of pressure placed on the palmar aspect of the finger tip to reduce the flexion deformity.
Mallet Deformity Injuries at Zone I can result in disruption of the attachment of the terminal extensor tendon from the base of the distal phalanx, the so-called mallet finger (Fig. 19.30). A mallet finger may be the result of laceration but is most commonly a closed injury as a result of forced flexion of the DIP in an extended digit. It can also result from a direct blow to the dorsum of the distal DIP joint or be secondary to a hyperextension force applied at the joint (1, 18, 35). With this mechanism of injury, structural failure may occur within the tendon, which is manifested by rupture at the osseous attachment with or without an avulsed bone fragment at the tendon insertion site (Fig. 19.31). Spontaneous disruption of the tendon has been described and may be the result of the blood supply of the terminal tendon. It seems that the extensor at the DIP has a zone of relative avascularity between 11 and 16 mm proximal to the insertion of the terminal tendon attachment. This is precisely the site where, with DIP flexion, the terminal tendon is stretched into contact with the head of the middle phalanx. The implication is that DIP flexion results in chronic repetitive stress and diminished vascularity in an already avascular structure (36).
Failure of the extensor tendon, whatever the mechanism, results in unopposed flexion of the joint. If left untreated, a mallet deformity will frequently progress to a swan neck deformity, the result of flexion deformity of the DIP joint together with hyperextension of the PIP joint caused by retraction of the extensor mechanism (Fig. 19.32) (35).
On MRI, the sagittal and axial planes are the most helpful for evaluating the course, quality, and integrity of the extensor tendon attachments. The patient may present with the finger in flexion at the DIP, the insufficiency of the terminal extensor tendon resulting in unopposed flexion. The diagnosis is made by discontinuity of the tendon proper or identification of the osseous avulsion injury. Any proximal retraction of the tendon from its native attachment should be noted.
Boutonniere Deformity The extrinsic extensor component of PIP extension is the central slip. This slip of the extensor tendon traverses the PIP and inserts as a wide band at the base of the middle phalanx as previously noted. Forceful blunt injuries, especially sharp, forced flexion against an extended finger, a blow to the dorsum of the middle phalanx, acute violent flexion of the PIP joint, or volar dislocation of the PIP joint, can result in this injury (Figs. 19.33–19.35) (18, 35). Much less frequently, it is associated with a fracture at the site of the central slip attachment. In the early acute phase, this diagnosis may be misleading. The injury to the central slip may not result in immediate loss of ability to extend the PIP as a result of the intact lateral bands, which serve as the primary extenders of this joint. The lateral bands must maintain a position dorsal to the axis of rotation of the joint to be effective in PIP extension. If the injury goes unrecognized (longer than 7 to 14 days), over time the lateral bands migrate to a volar position relative to the axis of rotation of the PIP joint. This occurs through continued PIP flexion in the absence of the central slip attachment. With volar migration of the lateral bands, they become flexors of the joint rather than extenders. The flexion at the PIP increases tension on the intact terminal extensor insertion to the base of the distal tuft (1, 37). As long as the lateral bands do not shorten, the PIP can be reduced to neutral position and can even be extended. With shortening of the lateral bands, however, the deformity becomes irreducible and fixed. The retinacular ligaments contribute to the fixation of this deformity in two ways: the retracted transverse fibers maintain the palmar dislocation of the lateral tendons and the oblique fibers secondarily contract, fixing the middle phalanx in flexion and the distal phalanx in extension (Figs. 19.36 and 19.37) (38). The chronic boutonniere deformity is one of the most difficult reconstructive problems to face for the hand surgeon (39).
As previously noted, a combination of axial and sagittal MR images best characterizes tendon abnormalities of the finger tendons. Like in the case of the mallet finger, the diagnosis of central slip failure is established by identifying discontinuity of the tendon fibers to the middle phalanx attachment site. Because one of the mechanisms of injury is dislocation, the PIP joint should also be assessed to identify any capsular injury. In addition to MRI, ultrasound has been established as an accurate and noninvasive study that can identify central slip injuries (40).
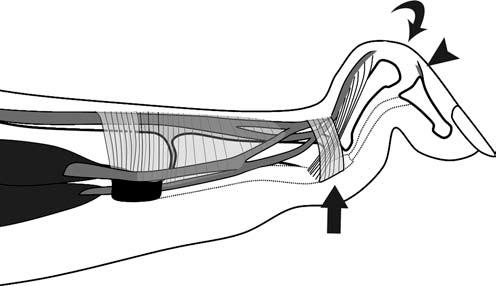
FIGURE 19.32 Diagram of the swan neck deformity. If an avulsion of the extensor tendon (arrowhead) is left untreated, the transverse and oblique retinacular ligaments of the proximal interphalangeal (PIP) joint can retract and scar down to a palmar position resulting in hyperextension at the PIP joint, exaggerating the unopposed flexion at the distal interphalangeal joint (curved arrow).
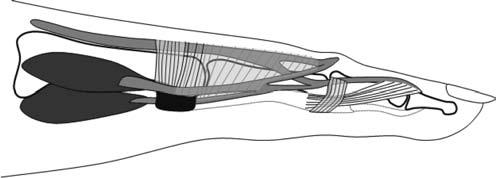
FIGURE 19.33 Diagram of the acute central slip injury. The central slip of the extensor tendon traverses the proximal interphalangeal and inserts at the base of the middle phalanx. Rupture of this tendon attachment, if undetected, can progress to a boutonniere deformity.
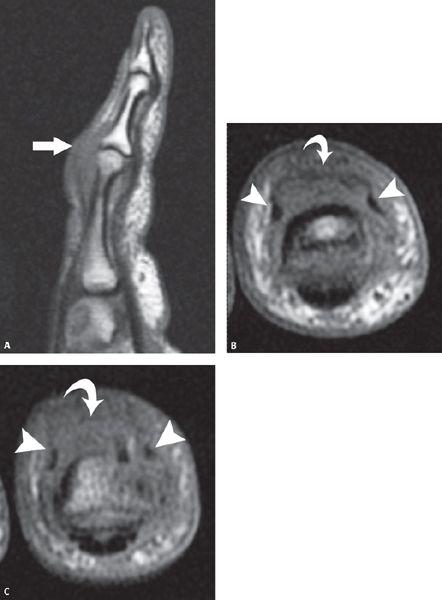
FIGURE 19.34 Acute central slip injury. T1-weighted sagittal MR image (A) shows intermediate signal intensity soft tissue prominence (arrow) at the dorsal surface of the finger adjacent to the proximal interphalangeal and base of the middle phalanx. No normal central slip is identified. Sequential T1-weighted axial MR images from proximal (B) to distal (C) show the absence of a central slip with intact lateral slips (arrowheads) consistent with an acute rupture.
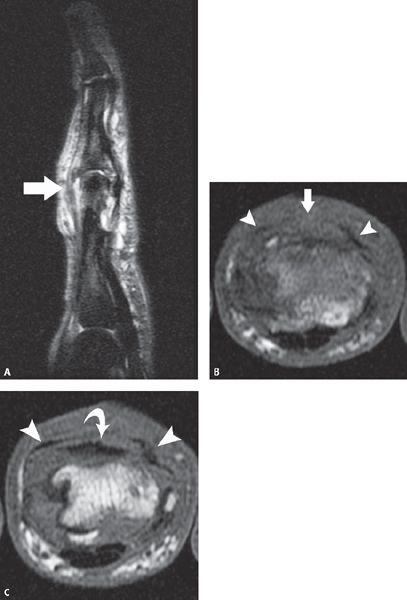
FIGURE 19.35 Acute central slip injury in the setting of degenerative changes of the proximal interphalangeal (PIP) joint. T2-weighted sagittal fat-suppressed MR image (A) shows thickening and irregularity of the central slip of the extensor tendon to the base of the middle phalanx (arrow) with surrounding edema in the soft tissues. Sequential T1-weighted axial MR images proximal to (B) and at the attachment site of the central slip (C) demonstrate the intact but slightly irregular lateral slips of the extensor tendon (arrowheads). Although the central slip is identified proximal to the PIP (curved arrow) (B), no normal structure is seen at the base of the middle phalanx (arrow) (C) consistent with an acute rupture.
Metacarpophalangeal (Zone V) Subluxation or Dislocation The extensor mechanism at the MCP joint is strongly fortified and not often subject to closed injuries. They do occur, however, and can be extremely painful with swelling and stiffness. The usual mechanism for closed injury in this region is a forceful crush or contusion-type injury that compresses the supporting structures of the joint against the underlying bone forcing the finger into flexion. The combination of forced flexion and ulnar deviation of the finger can also produce a closed injury at the MCP joint (1, 35). The injury is generally in the form of a capsular split or tear of the sagittal band retinacular fibers. Subluxation or dislocation of the extensor digitorum tendon at the MCP joint is the result of this insufficiency of the sagittal bands of the extensor hood. Patients present with an inability to completely extend the MCP joint. In the chronic setting, there may be a history of pain and swelling at the MCP joint with a snapping sensation in the finger.
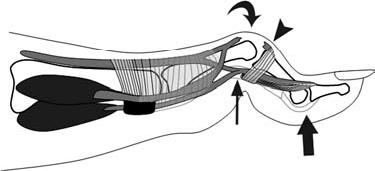
FIGURE 19.36 Diagram of a boutonniere deformity. In the setting of an undetected central slip injury (arrowhead), over time the transverse and oblique retinacular ligaments at the proximal interphalangeal (PIP) joint migrate to a palmar position (thin arrow) resulting in flexion at the PIP joint (curved arrow) and extension at the distal interphalangeal (thick arrow). This pattern of alignment is referred to as a boutonniere deformity.
MRI allows direct visualization of the position of the tendon relative to the MCP joint, more specifically relative to the metacarpal head. It also allows evaluation of tendon quality. Subluxation and dislocation are best appreciated in the axial imaging plane. MRI also allows direct assessment of the components of the extensor hood, in particular the sagittal band. In the acute setting, however, the presence of extensive soft tissue edema and swelling may obscure visualization of the structures in question. The diagnosis and characterization of sagittal band injuries are discussed in greater detail in the finger ligament Chapter.
Extensor Pollicis Longus Rupture Rupture of the extensor pollicis longus results in more functional loss than any other extensor tendon injury (Fig. 19.38) (41). Extensor pollicis longus rupture has been associated with chronic friction at Lister’s tubercle. Friction may also develop secondary to mass effect from an accessory extensor pollicis longus muscle within the third extensor compartment (27, 42). Degenerative or posttraumatic spurring of Lister’s tubercle as well as synovitis associated with rheumatoid arthritis or lupus are predisposing factors. In rheumatoid arthritis, the most common ruptures of tendons of the hand include the extensor pollicis longus and the extensor tendons of the little finger.
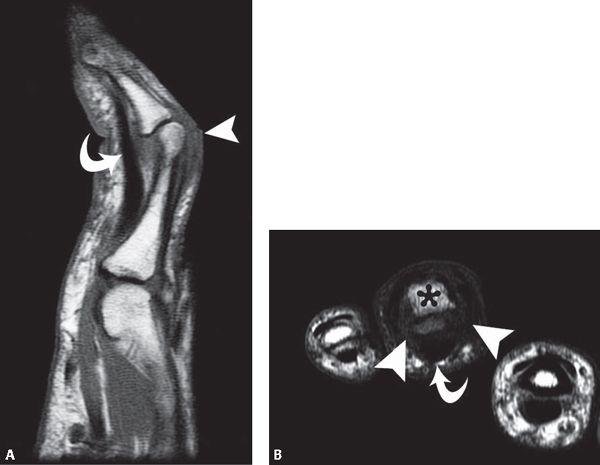
FIGURE 19.37 Boutonniere deformity. T1-weighted sagittal MR image (A) through the finger shows the intact flexor tendon (curved arrow) with flexion at the proximal interphalangeal joint. Although the proximal extent of the central slip can be seen anterior to the proximal phalanx, no discrete attaching fibers are present (arrowhead). T1-weighted axial MR image (B) through the base of the proximal phalanx (asterisk) demonstrates palmar migration of the lateral slips of the extensor tendon, increased intermediate signal intensity tissue in the region of the palmar capsule (arrowheads) and expected position of the displaced and thickened oblique retinacular tissue, and an intact flexor tendon (curved arrow).
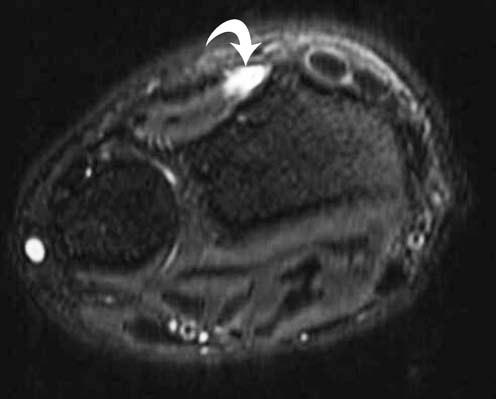
FIGURE 19.38 Rupture of the extensor pollicis longus. T2-weighted fat-suppressed axial MR image at the level of the distal radial ulnar joint show an empty third extensor compartment consistent with a rupture of the extensor pollicis longus.
The association of extensor pollicis longus tendon lesions and distal radial fractures is well established in the literature (27, 43, 44). Typically the fractures are minimally or nondisplaced (Fig. 19.39). The rupture occurs most often distal to the extensor retinaculum in an area of the tendon found to be hypoperfused on microvascular studies (43). Tendon rupture generally occurs 3 weeks to 3 months after the radial fracture. Like in all tendon ruptures, it is important to identify the torn ends of the tendon, localize them, and measure the gap. In acute cases, fluid within the tendon sheath will outline the tendon ends. In the setting of a chronic tear, however, the presence of scar tissue or fibrosis can fill in the tendon gap and obscure visualization of the ends of the tendon.
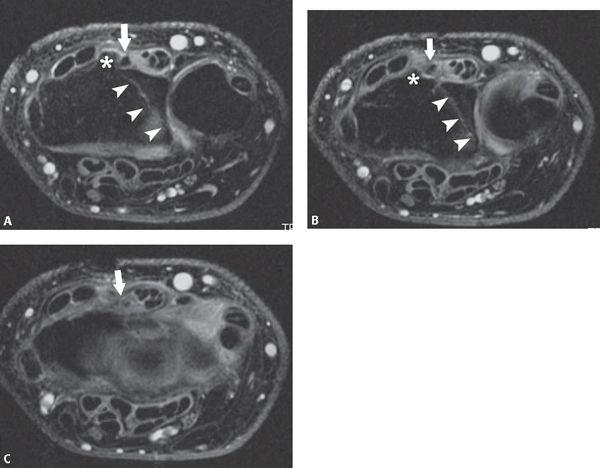
FIGURE 19.39 Rupture of the extensor pollicis longus with distal radius fracture. T2-weighted fat-suppressed axial MR image (A) shows a nondisplaced distal radial fracture (arrowheads). The extensor pollicis longus in the third extensor compartment (arrow) is noted adjacent to Lister’s tubercle (asterisk). Sequential distal T2-weighted fat-suppressed axial MR images show slight attenuation of the extensor pollicis longus (B) with discontinuity of the overlying tendon sheath with a rupture of the extensor pollicis longus (C) at the level of the joint line. Posttraumatic synovitis is evident at this level.
Rheumatoid Extensor Tendon Ruptures Rheumatoid arthritis is a disease of synovium. The disease affects both synovial-lined joint spaces and synovial-lined tendon sheaths. Tendons surrounded by inflamed synovium may become thickened, ruptured, or weakened. The extensor tendons are enveloped by tenosynovium as they course deep to the extensor retinaculum. The tenosynovium may extend distal to the extensor retinaculum by 2 to 4 cm into the six extensor compartments of the wrist. Dorsal tenosynovitis may involve any of the six compartments.
Synovitis as a cause of tendon rupture has been recognized for many years. The extensor pollicis longus drummers palsy, initially misdiagnosed as a paralytic condition, was eventually recognized as a true tendon rupture caused by synovitis (45). Tendon rupture has been associated with synovitis of syphilis, gonorrhea, and tuberculosis (46). Many cases of tendon rupture in the setting of rheumatoid arthritis have been described (45, 47, 48). The cause of tendon rupture appears to be the result of the effect of tenosynovitis on the tendon itself and not the mechanical irritation of the tendon on adjacent bone. Furthermore, the tenosynovitis has been reported to interfere with the blood supply of the tendon, there by altering tendon integrity and causing tendon necrosis (12, 46). Tenosynovitis of finger flexor and extensor tendons in rheumatoid arthritis occurs in up to 64% of all patients with rheumatoid arthritis, more often in extensor than in flexor tendons (41).
Single tendon ruptures, as noted previously, typically affect either the extensor pollicis longus or the extensor digiti minimi. Extensor pollicis longus ruptures usually occur at Lister’s tubercle. Although the extensor pollicis longus injury does not usually progress to other digits, the rheumatoid-related extensor digiti minimi rupture does. In the setting of double extensor tendon ruptures, the ring and little fingers are commonly involved. Both MRI and ultrasound have proven helpful for the diagnosis of tendon abnormalities in the setting of rheumatoid arthritis (41). The MRI findings of tenosynovitis are discussed in greater detail later in this Chapter.
Flexor Tendon Injuries
Traumatic Injuries
Injuries to the flexor tendons are not as common as those encountered in the extensor tendons. A variety of etiologies and associated conditions have been proposed in the setting of the nontraumatic flexor tendon rupture, including Von Recklinghausen’s disease, systemic lupus erythematosus, gout, Kienböck’s disease, iatrogenic injury, electrical injury as well as idiopathic rupture (49–54). The unique anatomic arrangement of the tendons and supporting structures at the palmar hand leads to complex injury in the setting of penetrating trauma. Similarly, however, lesions in the flexor system can be classified with respect to lesion location or subdivided into open or closed injury. To briefly review, Zone I is the area distal to the insertion of the FDS tendon on the middle phalanx. Zone II is the area from the palmar plate of the MCP to the FDS insertion. Zones III, IV, and V are the remainder of the hand and wrist, encompassing the areas distal to, at, and proximal to the carpal tunnel, respectively.
Open Injuries
In the flexor tendon system, open injuries in the form of lacerations with skin wounds are more common than closed traumatic ruptures (Fig. 19.40) (1). Although the diagnosis is usually made clinically, the physical signs of injury can be nonspecific. In clinical practice, suspected partial tendon lacerations have been explored surgically as a result of the lack of a reliable method to prospectively predict the extent of injury. MRI has been shown to accurately distinguish different degrees of flexor tendon tears (55).
In the majority of cases, these types of lesions occur in midsubstance of the tendon rather than at sites of osseous attachment (1, 56). Injuries in Zone I (middle to distal phalanx) are isolated lacerations of the FDP and manifest as loss of active flexion of the distal phalanx. Trauma to the four proximal zones implies lesions of both FDS and FDP with resultant loss of active flexion of both the PIP and DIP joints. Trauma in the proximal three zones is often complicated by injuries to major neurovascular structures and the lumbricals in addition to the flexor tendons (57). Lacerations in Zone II (middle phalanx to proximal palmar fold) are the most frequent and carry the most severe prognosis (1, 58). Scar material that forms within the flexor sheath can lead to adhesions, entrapment, or triggering of the flexor tendons (Fig. 19.41) (55, 59–61). Bunnell called Zone II “no man’s land” and warned against attempts to repair flexor tendon injuries in this region (55). Verdan (61) subsequently demonstrated that complete lacerations could be successfully treated by primary repair.

FIGURE 19.40 Laceration of the flexor tendon. T2-weighted sagittal MR image through the finger shows focal discontinuity of the flexor tendon of the finger. There is minimal gap between the torn ends of the flexor digitorum superficialis (curved arrow) with a greater gap between the ends of the flexor digitorum profundus. The sharp, horizontal margins of the torn tendon ends and the lack of tendinosis suggest laceration as the mechanism of injury.
Rubin et al. (55) established the usefulness of MRI for the diagnosis of both partial and complete lacerations of Zone II flexor tendon lesions in a cadaveric model. In this study, injuries were correctly characterized as complete, low-, or high-grade lesions. If a complete tendon disruption was noted, the gap between the torn ends was reported. The distinction between low-and high-grade partial tears was established based on the percentage of total tendon cross-sectional area that was disrupted. Tears that involved less than 50% of the total tendon area were defined as low-grade lesions, and those that involved 50% or more were considered high-grade partial tears. Although complete lacerations are often obvious clinically, MRI can be useful to identify the degree of retraction, if any, in a complete rupture. Moreover, in some cases, complete tendon rupture can mimic a partial laceration when an intact vinculum (small synovial band encompassing a vessel that emanates from the digital artery and affords vascular supply to the tendon) prevents proximal retraction of the tendon, there by preserving some degree of active flexion (60).
The MRI diagnostic criteria and characterization of such lesions parallel that of similar lesions in the extensor system. In the flexor system, however, the fixation system of tendon to adjacent bone is not as strong as that of the extensor system. For this reason, a higher degree of retraction may be encountered in the setting of injury. In addition, the gap between torn ends of tendon may be overestimated if the tendon is curled or overlaps itself (1).
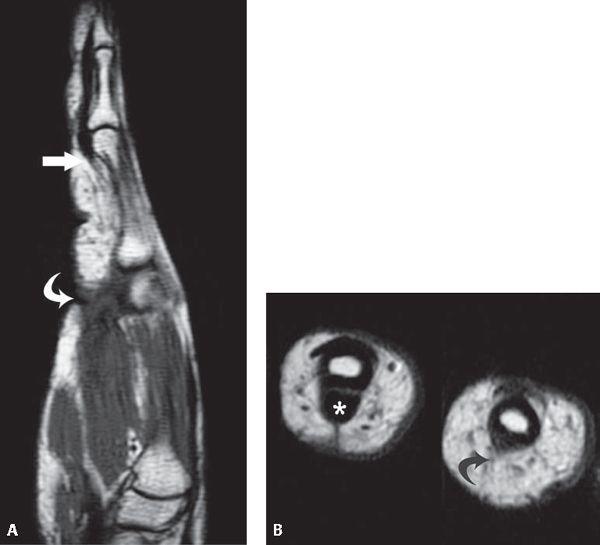
FIGURE 19.41 Remote flexor tendon rupture. T1-weighted sagittal MR image (A) through the finger profiles the gap between the torn and scarred proximal (curved arrow) and distal ends (arrow) of the flexor tendon. Corresponding T1-weighted axial MR image (B) through the fingers shows the absent flexor tendon (curved arrow) with a normal flexor tendon (asterisk) in the adjacent finger. The absence of signal changes in the subcutaneous fat supports the history of a remote injury.

FIGURE 19.42 Flexor tendon rupture. T1-weighted sagittal MR image (A) profiles the flexor tendon to the level of the metacarpophalangeal (MCP) joint (arrow) where it shows a somewhat irregular contour. Corresponding T1-weighted axial MR images at the level of the MCP track the tendon from a relatively normal appearance (B) (arrow) to a complete rupture (C) (arrow). Marginal erosions (curved arrows) are identified in the axial imaging plane (C) but better profiled on a T1-weighted coronal MR image through the fingers (D).
Although no study to date has compared MR pulse sequences for evaluation of flexor tendon lacerations, some advocate the use of three-dimensional gradient recalled echo images emphasizing the advantage of reformatted images in lesion diagnosis and characterization (55). In the acute setting, hemorrhage and edema associated with the injury would be optimally detected with a fluid-sensitive sequence keeping in mind that these harbingers of acute injury could also obscure anatomic detail obviating the potential distinction between low- and high-grade lesions.
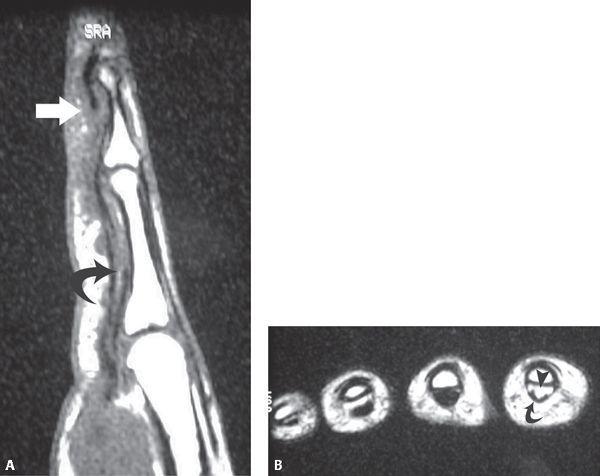
FIGURE 19.43 Closed rupture of the flexor digitorum profundus. T1-weighted sagittal MR image (A) shows a rupture of the flexor digitorum profundus with the distal (arrow) and proximal ends (curved arrow) of the ruptured tendon noted. T1-weighted axial MR image (B) nicely demonstrates the absence of the flexor digitorum profundus (arrowhead) with the intact, superficial flexor digitorum superficialis in place (curved arrow).
Closed Injuries
Closed tendon injuries include avulsion of the FDP and FDS tendons. These injuries are uncommon primarily as a result of the fact that the tendon is considered the strongest part of the flexor musculotendinous unit (Fig. 19.42) (62). Often, there is a chronic pathologic condition such as rheumatoid arthritis, osteoarthritis, or previous trauma that weakens the tendon (63–68). Acute sports injuries may also be responsible for the closed flexor tendon injury.
Avulsion of the FDP tendon is the most frequent type of closed rupture and is caused by a sudden hyperextension injury during active flexion. This mechanism is often referred to as the “jersey finger” (1, 69). It is the FDP tendon of the ring finger that is most commonly injured, and several hypotheses for this have been suggested. It has been suggested that the common flexor muscle belly of the profundus of the middle, ring, and little fingers makes the ring finger more susceptible to this injury. The anatomic arrangement of the extensor tendons may also play a role. When the metacarpal joints of the middle and little fingers are flexed to 90 degrees, the ring finger cannot be fully extended. The ring finger extensor is pulled distally by the junctura tendineae as the middle and little fingers flex. This acts as a check rein to prevent passive extension of the ring finger, making it more susceptible to hyperextension injury or to flexion against a resisted force, which can result in avulsion of the profundus insertion. In addition, it has been shown that the breaking strength of the FDP of the ring finger is significantly less than that of the middle finger (69, 70).
This is an important imaging diagnosis because it can be easily overlooked in the acute setting. There is no classic deformity or alignment abnormality associated with it on physical examination, and the combination of pain and soft tissue swelling may mask the pathognomonic sign of loss of active flexion at the DIP joint. In each case of tendon rupture, it is important to know the size of the gap between the torn ends of the tendon, the location of the proximal end, and the appearance of the tendon. Classically, the length of the gap between the tendon ends is an essential element in the decision regarding treatment. If the gap is more than 30 mm, a tendon graft is preferred to a single suture of the tendon ends (71, 72). MRI has been shown to be useful in ascertaining this information (Fig. 19.43) (73). Drapé et al. (73) found that axial T1-weighted spin echo and three-dimensional gradient echo acquisitions were generally sufficient to evaluate the appearance of the ruptured tendon. In some cases, a second centering was necessary when the proximal end of the tendon was not initially visible. In a series of 10 patients with 12 flexor tendon ruptures, MR images accurately depicted the level of the rupture, the gap between the tendon ends, and the position of the proximal tendon retraction. In two cases, MRI was able to delineate a palmar mass as a retracted tendon rather than the clinically suspected ruptured lumbrical muscle. The intravenous injection of a gadolinium-based contrast material was not shown to provide new or more specific diagnostic findings.
Four main variations of the ruptured FDP have been described based on the level of the lesion, the degree of retraction, and the presence or absence of an osseous fragment. Type I lesions are characterized by retraction of the tendon into the palm. Type II lesions show tendon retraction to the PIP joint with or without a small osseous avulsion at the joint. In Type III lesion, there is an avulsion of a large osseous fragment that remains in situ. Type IV lesion demonstrates failure at the bone with a fracture fragment noted at the tendon attachment site as well as failure of the tendon attachment to bone with a concomitant detachment of tendon from fracture fragment (1, 74).
Isolated avulsion of the FDS is uncommon with most reported cases occurring in conjunction with FDP tendon injuries (1, 56). Injury to the FDS occurs with forced extension in the actively flexed finger. This diagnosis is suggested on physical examination by the inability to independently flex the PIP joint. The patient also exhibits palmar tenderness with a palpable mass and limited ability to fully extend the PIP and DIP joints. Commonly, like in FDP avulsions, the diagnosis is delayed (74).
Flexor Pollicis Longus Rupture Rupture of the flexor pollicis longus tendon may develop from chronic friction against the scaphoid. This can occur in the setting of rheumatoid arthritis or with volar carpal subluxation. It is important to identify the torn tendon end because the flexor pollicis longus does not have either a vincula or lumbrical. This allows the tendon to retract freely (27). Complete rupture may be preceded by tendinosis and superimposed partial tears (Fig. 19.44).
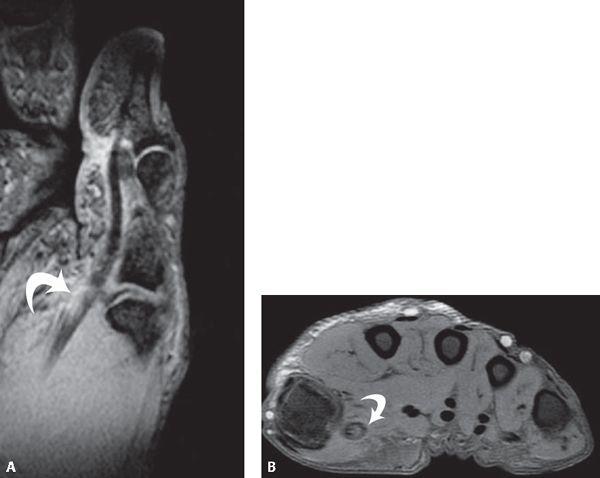
FIGURE 19.44 Partial tear of the flexor pollicis longus. Gradient oblique sagittal MR image (A) through the thumb show abnormal thickening of the flexor pollicis longus (curved arrow) with high internal signal intensity consistent with partial tear. Corresponding axial MR image (B) verifies the thickening and increased internal signal intensity (curved arrow) within the tendon.
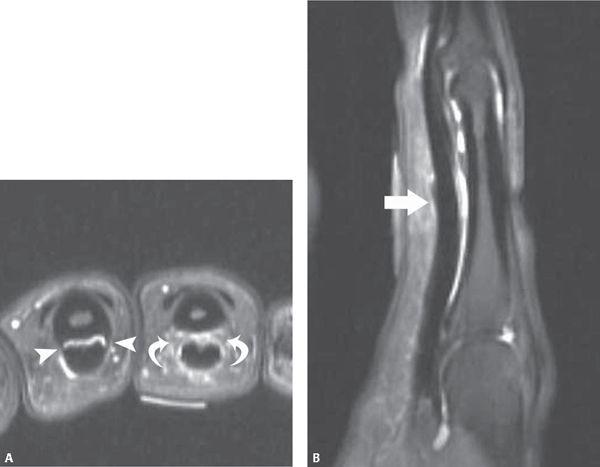
FIGURE 19.45 Digital A2 pulley rupture. Proton density-weighted fat-suppressed axial MR image (A) at the level of the proximal phalanx show the absence of the linear low-signal–intensity pulleys (curved arrow) extending from the flexor tendon to the bone. The normal appearance of the pulleys (arrowheads) is noted in the adjacent finger. T2-weighted fat-suppressed sagittal MR image (B) through the proximal phalanx demonstrates edema around a thickened portion of the A2 pulley (arrow). Note there is no increased gap between the tendon and the bone, making the axial images of paramount importance in the diagnosis of pulley rupture.
Flexor Carpi Radialis Rupture Rupture of the flexor carpi radialis tendon can occur as the result of falling on the outstretched hand, causing an avulsion at its insertion with or without an osseous fragment. Chronic partial tearing can also be encountered in the setting of osseous spicules emanating from the scaphotrapezial joint as seen with degenerative changes.
Flexor Tendon Repair Complications
The restoration of an injured digital flexor tendon to a functional state after its repair remains a challenging task for the clinician. Clinical evaluation of the flexor tendon repair can be difficult as a result of the insidious onset of tendon rupture. Two important complications that can prevent active flexion of the finger include breakdown of the tendon repair and the development of adhesions in the digital canal (75, 76). In one study, clinical examination of the repaired flexor tendon rupture yielded 60% accuracy in the diagnosis of a tendon rupture, whereas MRI offered 100% accuracy in this endeavor (77). Not only are treatment options markedly different for these complications, but postoperative course is drastically different in terms of rehabilitation as well as duration of incapacity. A large retear is treated with staged tendon grafting, whereas tenolysis is used in cases of adhesions (75).
In a study by Drapé et al. (75), 51 patients who had undergone repair of 64 flexor tendon injuries without recovery of active finger flexion were evaluated. Locations of the injuries included seven Zone I, 42 Zone II, and eight Zone III lesions in the fingers. There were three Zone I, three Zone II, and a single Zone III lesion in the thumb. In the study, MRI was successful in distinguishing between the complications that occurred after tendon repair (75).
Frank tendon rupture was easily depicted and occurred in 22% of the fingers studied (73). MRI provided additional information on the length of the gap between the torn tendon ends, the level of the proximal tendon end, the amount of associated adhesions, and the state of the pulleys. Restoration of flexor tendon performance is difficult if MRI reveals a badly scarred digital canal with deficient pulleys and a long tendon gap (78).
MRI was also helpful in characterization of the tendon repair site. Elongation of callus at a site of tendon repair is very frequent and is considered physiological if it does not exceed a certain length. Callus is identified as the heterogeneous tissue between the torn ends of the tendon. Elongation of up to 5 mm does not exclude a good outcome; however, if callus at the tendon exceeds 10 mm in length, reorganization of the tendon is not possible and reoperation with tendon grafting is often necessary. Graft elongation was noted in 29% of failed tendon repairs in this series of patients (73). In addition, intermediate signal intensity of the tendon repair site can indicate the presence of immature callus.
Even in the setting of an optimal technical tendon repair, adhesions often result. Peritendinous adhesions accounted for 49% of failed tendon repairs in the series of Drapé et al. (73). Isolated peritendinous adhesions were diagnosed when the tendon appeared continuous, had strongly predominant low-signal–intensity collagen fibers on axial sections, and had associated thickening of the tendon sheath or peritendinous soft tissues.
Pulley System Injuries
As previously noted, finger flexion relies heavily on the delicate focal thickened areas of the flexor tendon sheath, referred to as the pulley system, as well as the flexor tendons proper to successfully elicit fine motor tasks. Such flexion requires proximal excursion of the flexor tendon and tight apposition of the tendon to adjacent osseous structures during this excursion, both of which are afforded by the pulley system. Lesions of the pulley system of the finger have been recognized with increasing frequency as a result of the growing popularity of activities such as rock climbing. Such activities impose extensive stress on the supporting structures of the hands and fingers. During rock climbing, the pulley system is exposed to high grip-specific loads of up to 700 newtons (79–82). Specifically, forceful flexion of the fingers with the MCP joint in extension, PIP joint in flexion, and DIP joint in extension can lead to extreme stress on the A2 and A3 pulleys and lead to ultimate failure in the form of rupture. Pulley ruptures related to climbing are most commonly seen in the ring and middle fingers. Early diagnosis of pulley ruptures is mandatory to prevent fixed contractures of the PIP joint.
Injury of the pulley system begins at the distal part of the A2 pulley, the strongest of the annular pulleys and most important for tendon function. With progression of the severity of injury, pulley lesions in the A3 and A4 position follow (1, 83, 84). Rarely is the A1 pulley injured.
In the past, the imaging diagnosis of pulley lesions was made by indirect means through the detection of a gap between the flexor tendon and the adjacent bone with the finger in forced flexion, the so-called bowstring sign. This sign reflects an extensive abnormality of the pulley system that leaves limited or partial lesions of the pulleys virtually undetected (22, 55, 73, 75, 85–89). Other investigators have shown that the A2 and A4 pulleys can be identified through direct visualization with both conventional MRI as well as ultrasound. On MR images, the nonvisualization of the pulley, best demonstrated in the axial imaging plane, establishes the diagnosis of a pulley rupture (Fig. 19.45). Lesions of the pulley system, as noted previously, can also be diagnosed indirectly by detection of a gap between the flexor tendon and the bone on sagittal images obtained during forced flexion. This has been referred to as the bowstring sign (Figs. 19.46 and 19.47). The degree and distribution of tendon displacement can suggest the severity and localization of pulley lesions. With maximal displacement at the proximal and middle phalanx, there are tears in the A2 and A4 pulleys, respectively. Incomplete disruption of the A2 pulley is diagnosed on sagittal MR images when bowstringing does not extend proximally beyond the base of the proximal phalanx. Conversely, proximal extension of bowstringing beyond the base of the proximal phalanx is indicative of a complete disruption (88, 90).

Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


