MR imaging has been optimized for the evaluation of a multitude of disease processes affecting the kidneys. A wide variety of noncontrast methods are available for the evaluation of both kidney structure and function, which are especially useful in clinical scenarios that obviate the use of intravenous contrast. Contrast-enhanced methods remain important, especially for tumor evaluation, and are used increasingly for functional analysis of quantitative biometrics, such as glomerular filtration rate and kidney blood flow.
Key points
- •
MR imaging is a widely used noninvasive method that has intrinsic strengths for evaluating a wide range of renal pathology and has the ability to provide functional analysis of the kidney (eg, renal blood flow, oxygenation and glomerular filtration rate), that is not practically available with any other imaging technology.
- •
There are a wide variety of noncontrast MR imaging techniques available for evaluating both kidney structure and function, which are especially useful in patients with reduced kidney function and obviate the use of intravenous contrast.
- •
Contrast-enhanced techniques improve diagnostic accuracy for a wide range of clinical indications, including tumor evaluation, and are used increasingly for functional analysis of quantitative biometrics, such as glomerular filtration rate and kidney blood flow.
Introduction
MR imaging is a widely used noninvasive imaging method that has intrinsic strengths for evaluating a wide range of renal pathology. Advantages of MR imaging include excellent soft tissue contrast and no ionizing radiation exposure. In addition, MR imaging has the ability to provide functional analysis of the kidney (eg, renal blood flow, oxygenation, and glomerular filtration rate), that is not practically available with any other imaging technology. Contrast-enhanced imaging is an important component of MR imaging examinations of the kidney. Although there are potential safety concerns with gadolinium-based chelate agent (GBCA) administration, the overall safety profile is excellent and, by comparison, favorable to iodinated contrast agents. In addition, there is a growing array of diagnostically useful noncontrast MR imaging techniques available. This review highlights the various noncontrast and contrast-enhanced MR techniques available for kidney imaging, and highlights their utility in clinical practice.
Noncontrast techniques
T2-Weighted Imaging
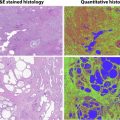
T2-weighted (T2W) imaging is a fundamental component of any abdomen-pelvis MR Exam, and for body imaging. Acquisition with a single-shot technique provides the most robust, high-quality fluid-sensitive imaging for renal pathology. Single-shot T2W sequences (ssT2) are truly the workhorse of noncontrast body MR imaging, and provide excellent structural and morphologic evaluation of the kidneys and collecting system. Compared with standard, multi-shot turbo spin-echo T2 images, ssT2 images can suffer from some image blurring due toT2 decay along the long readout as well as the use of partial Fourier acquisition to reduce specific absorption rate (SAR). Multi-breath-hold T2 fast spin-echo (T2 FSE) sequences are another option, which have the advantage of increased image sharpness and some improvements in T2 contrast between lesions and normal tissues. However, the need for multiple breath holds increases the time and complexity of the examination, and is not possible in patients who have difficulty in breath-holding. By using the single-shot technique, robust image quality can be performed even in free-breathing patients, ideal for patients of varying levels of cognition and health status. Recently, the image quality of ssT2 sequences has been significantly improved by using a variable refocusing flip angle methodology, which has the combined benefit of increasing image sharpness and also decreasing SAR and scan times ( Fig. 1 ).
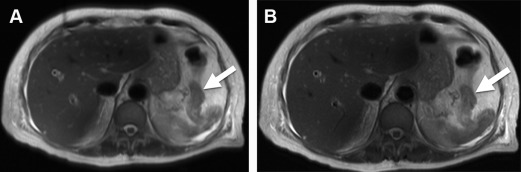
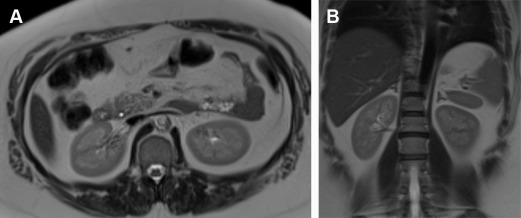
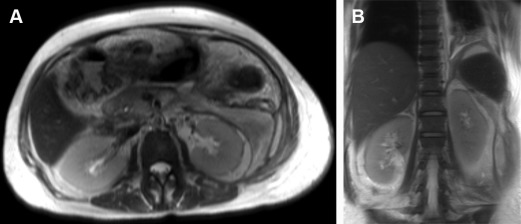
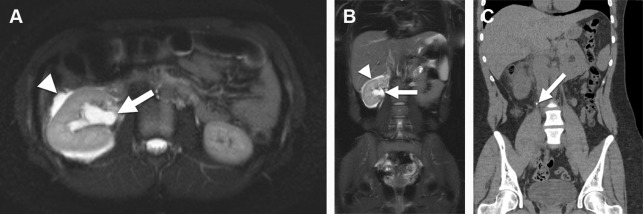
T2W imaging is key for differentiation of the normal renal cortex and medulla ( Fig. 2 ), a differentiation that is lost in both acute and chronic kidney disorders ( Fig. 3 ). The bright signal intensity of fluid in T2W MR imaging is excellent for depiction of the renal collecting system, and provides a highly sensitive method for evaluating hydronephrosis. Although MR imaging is not sensitive for the detection of calcified urologic stones, it is highly sensitive for the secondary changes of obstruction and perinephric fluid that occurs with obstructing urolithiasis ( Fig. 4 ), correctly identifying the source of pain in patients who may want to avoid exposure to ionizing radiation, such as pregnant and pediatric patients.
Diffusion-Weighted Imaging
Diffusion-weighted imaging (DWI) is based on the Brownian motion of water molecules and used to distinguish between the rapid, unrestricted diffusion of protons versus impeded or slow diffusion of protons (restricted diffusion). The impendence of water molecules is related to high tissue cellularity and the presence of intact cell membranes, whereas unrestricted diffusion is associated with low tissue cellularity that permits rapid diffusion of protons. Therefore, restricted diffusion is most often identified in highly cellular tumors, cytotoxic edema, abscesses, and fibrosis. Apparent diffusion coefficient (ADC) maps are generated from diffusion images obtained at different b values and provides a quantitative metric of differences in tissue diffusivity.
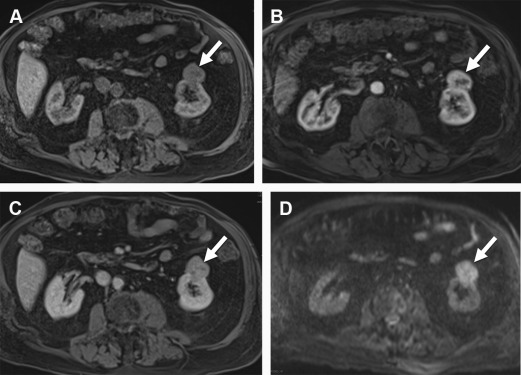
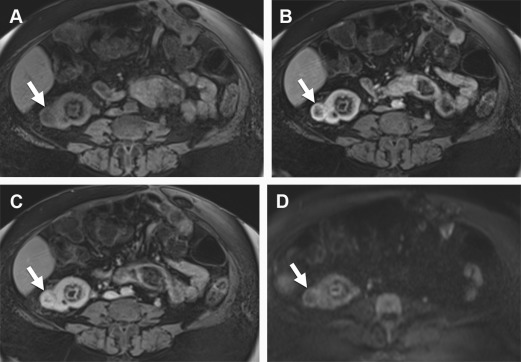
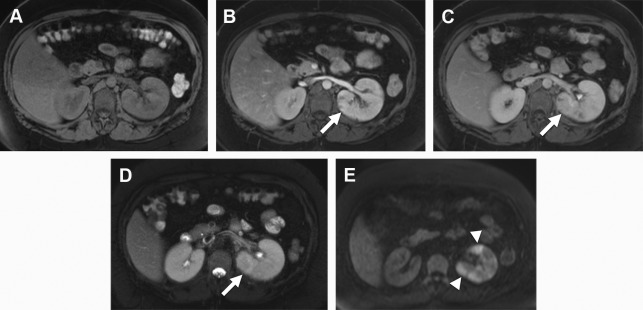
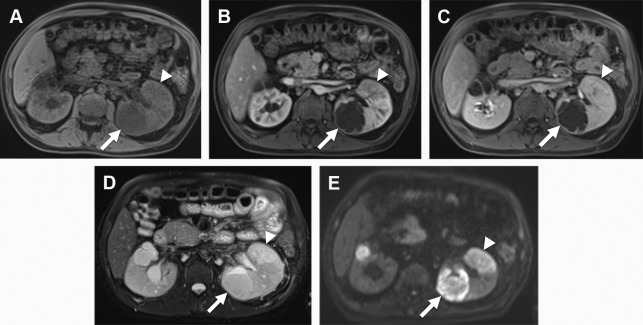
The addition of DWI in abdominal imaging protocols has become standard over the past decade, with an oncologic emphasis based on a high sensitivity for the detection of early metastatic disease in a variety of tumor subtypes. DWI is relatively less useful for the primary diagnosis of renal cell carcinoma (RCC), due to a lower contrast differentiation between RCC and normal renal parenchyma (compared with hepatic tumor demonstration, for example). However, there has been extensive work investigating the diffusion characteristics of benign versus malignant renal masses, subtyping RCCs, and tumor grading. Multiple studies have suggested that malignant renal tumors may demonstrate statistically significant lower ADC values as compared with benign lesions ( Figs. 5 and 6 ). A meta-analysis based on 17 studies with 764 patients showed that RCCs have significantly lower ADC values than benign tissue (1.61 ± 0.08 × 10 −3 mm 2 /s versus 2.10 ± 0.09 × 10 −3 mm 2 /s; P <.0001). Sandrasegaran and colleagues determined that ADC measurements may aid in differentiating benign cystic lesions from cystic renal cell cancers. They found that ADC values of the benign lesions were significantly higher than those of the malignant lesions (mean, 2.72 vs 1.88 × 10 –3 mm 2 /s; P <.0001); the ADCs of the 31 benign cysts were significantly higher than those of the 7 cystic renal cancers (2.77 vs 2.02 × 10 –3 mm 2 /s; P <.001).
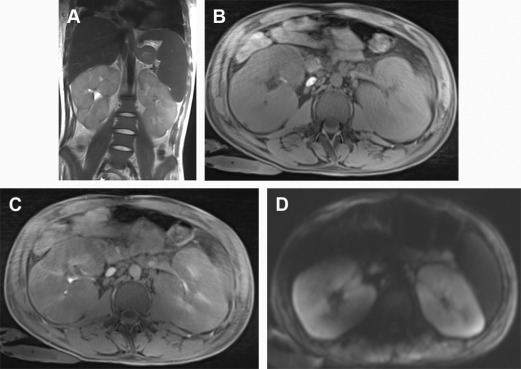
The diagnosis of lymphoma is a clinical scenario in which DWI has significant added benefit, as lymphomatous tissue demonstrates markedly restricted diffusion (especially compared with background renal parenchyma), providing some added diagnostic specificity for this tumor type ( Fig. 7 ).
In addition, DWI is very useful in the assessment of pyelonephritis and abscess. In pyelonephritis, DWI demonstrates a striated pattern of restricted diffusion ( Fig. 8 ) that may demonstrate abnormality even before contrast-enhanced images. Abscesses form as a later sequelae of severe pyelonephritis, and manifest as a fluid-filled cavity in the renal parenchyma that demonstrates marked restricted diffusion ( Fig. 9 ), which allows for ready differentiation from renal cysts. Rathod and colleagues examined the role of DWI in diagnosing infection and found that areas of nephritis had significantly lower ADC values than the normal renal cortical parenchyma. Also, renal abscesses had significantly lower ADC values than areas of nephritis. In a retrospective study of 88 patients, Goyal and colleagues found that abscesses and RCC both show statistically significant restricted diffusion as compared with the renal parenchyma (1.12 and 1.56, respectively, vs 2.34 ×10 −3 mm 2 /s for normal kidney; P <.0001 for both), and abscesses restricted to a greater extent than RCCs, which was also statistically significant.
Angiography
Several noncontrast MR angiography techniques have been developed in the past decade, which use either flow-related enhancement, phase-dependent enhancement, or flow-independent enhancement. The most common noncontrast MR techniques to image the renal vasculature include time of flight (TOF), inflow-balanced steady-state free precession (SSFP), and phase contrast.
In conventional TOF angiography, the background stationary volume in an imaging slab is saturated, whereas the inflowing fresh blood appears bright. Although this technique is prevalent for evaluation of the intracranial vasculature, TOF is challenging in renal imaging due to of the limited saturation of vessels with in-plane flowing blood, respiratory motion artifacts, arterial pulsation artifacts, and signal loss at severe stenoses.
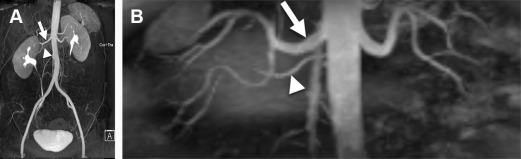
SSFP angiography is a flow-independent bright blood technique deriving image contrast from the T1 and T2 properties of blood pool. SSFP is based on a gradient-echo (GRE) sequence in which steady-state longitudinal and transverse magnetizations are maintained. This technique uses a slab selective adiabatic inversion pulse to suppress the stationary background tissue. The long inflow time of several hundred milliseconds ensures adequate inflow of fresh arterial blood into the imaging slab, which imparts a high signal-to-noise ratio (SNR). Given that this method relies on brisk arterial inflow, it is suboptimal in individuals with slow flow or poor cardiac output. Advantages of this SSFP are high SNR, shorter acquisition times, and widespread availability; this technique has been used for the preoperative evaluation of renal donors to depict renal vascular anatomy ( Fig. 10 ). Limitations of the technique are susceptibility to field heterogeneity and interference from background signals requiring additional preparatory pulses.