Presentation and Presenting Images
( ▶ Fig. 13.1, ▶ Fig. 13.2, ▶ Fig. 13.3, ▶ Fig. 13.4, ▶ Fig. 13.5, ▶ Fig. 13.6)
A 58-year-old female with a history of Crohn’s disease presents for routine screening mammography.
13.2 Key images
( ▶ Fig. 13.7, ▶ Fig. 13.8, ▶ Fig. 13.9, ▶ Fig. 13.10)
13.2.1 Breast Tissue Density
The breasts are heterogeneously dense, which may obscure small masses.
13.2.2 Imaging Findings
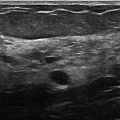
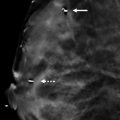
The imaging of the left breast is normal (not shown). The right breast demonstrates multiple obscured masses with a dominant mass (circle) at the 5 to 6 o’clock location. This mass is well-circumscribed on both conventional mammographic ( ▶ Fig. 13.7, ▶ Fig. 13.8) and tomosynthesis imaging ( ▶ Fig. 13.9, ▶ Fig. 13.10). The tomosynthesis images further define the margins of the smaller lesions (best seen on the tomosynthesis movie). The dominant mass is stable compared to prior mammographic evaluations ( ▶ Fig. 13.5, ▶ Fig. 13.6) and its borders are well-circumscribed on conventional mammographic imaging.
13.3 BI-RADS Classification and Action
Category 2: Benign
13.4 Differential Diagnosis
Cyst: Cysts are often multiple, usually bilateral, and may be painful and fluctuate in size. They are most common in 30- to 50-year-old patients. Cysts can appear as well-circumscribed masses.
Fibroadenoma: Fibroadenomas are the most common benign masses in young women. They may be multiple in 10 to 15% of patients. Fibroadenomas can appear as well-circumscribed masses.
Breast cancer: Breast cancer may present as a well-circumscribed mass; however, it is much less common. Careful evaluation of imaging characteristics is necessary, and, if there is doubt, then additional diagnostic imaging should be performed including an ultrasound.
13.5 Essential Facts
By definition, the term multiple bilateral masses refers to at least three masses total with at least one mass in each breast.
Multiple obscured or partially obscured masses have margins hidden by overlying breast tissue. Tomosynthesis and ultrasound are helpful to define the margins of these masses.
Leung and Sickles (2000) found that the frequency of cancer development and the stage of cancer diagnosis in patients not recalled for multiple bilateral breast masses are similar to those seen in the general screening population. The authors concluded that recall for multiple masses did not appear to be justified.
To be considered partially circumscribed, at least 75% of the margins should be circumscribed and the remaining 25% should be obscured. No portion of the margins should be considered indistinct.
13.6 Management and Digital Breast Tomosynthesis Principles
In the study by Rafferty and colleagues (2013), it was discovered that care must be taken to avoid misclassification of malignant lesions. Some cancers seen on tomosynthesis as circumscribed lobular masses were being dismissed by some readers. This is because radiologists most often associate circumscribed masses with benign or probably benign lesions.
In this case each mass could be evaluated individually.
The slices on tomosynthesis reduce or eliminate breast tissue overlap and structural noise seen in single slice conventional mammographic imaging. Only findings on the imaged section appear sharp, whereas those above or below appear out of focus. This allows each lesion to be carefully assessed independent from the other lesions or distractions in the breast tissue.
Tomosynthesis reduces callbacks for benign findings but increases interpretation time.
13.7 Further Reading
[1] Leung JW, Sickles EA. Multiple bilateral masses detected on screening mammography: assessment of need for recall imaging. AJR Am J Roentgenol. 2000; 175(1): 23‐29 PubMed
[2] Rafferty EA, Park JM, Philpotts LE, et al. Assessing radiologist performance using combined digital mammography and breast tomosynthesis compared with digital mammography alone: results of a multicenter, multireader trial. Radiology. 2013; 266(1): 104‐113 PubMed

Fig. 13.1 Right craniocaudal (RCC) mammogram.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


