Abstract
Muscles and nerves may demonstrate benign physiologic FDG avidity and must be distinguished from malignancy. This chapter describes common appearances of benign FDG avidity in muscles and nerves and compares them to the appearance of malignancy.
Keywords
FDG, PET/CT, muscle, nerve
Muscles are a less common site of malignancy, yet are very important to the proper interpretation of 18F-flourodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) in their own right. Benign skeletal muscle may demonstrate substantial FDG uptake, and this should not be confused with malignancy. Physiologic FDG avidity in skeletal muscle is often related with muscular exertion, which is why at most FDG PET facilities patients are asked to refrain from exercise the day before and the day of a PET/CT scan. Linear FDG avidity corresponding to normal appearing muscles on CT is usually physiologic ( Fig. 4.1 ).
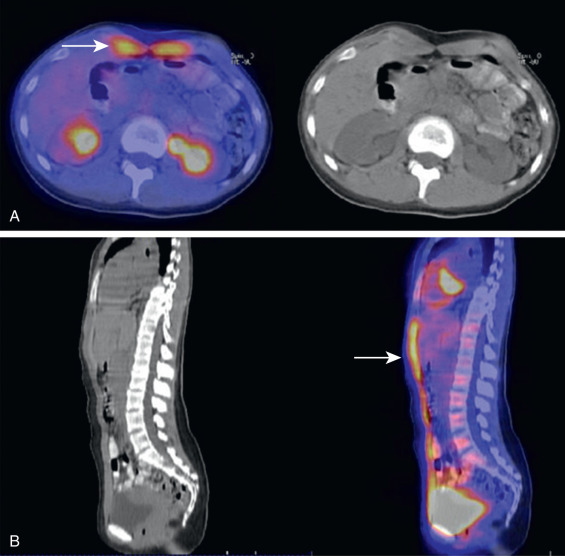
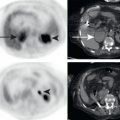
Extensive physiologic FDG avidity could initially be alarming on PET/CT examinations. For example, large segments of FDG-avid back musculature are uncommon and could mimic an aggressive process. However, correlation with the corresponding CT images usually allows for the proper identification of physiologic muscular FDG avidity. Note the patient in Fig. 4.2 . This patient has extensive FDG avidity in the region of back musculature. The corresponding CT images demonstrate normal fat planes within the FDG-avid muscle, consistent with benign muscle, despite the extensive FDG avidity. FDG-avid masses would be expected to displace or obliterate the normal fat planes within musculature ( Fig. 4.3 ). While areas of FDG-avid malignancy underlying the physiologic muscular FDG avidity cannot be entirely excluded, the presence of normal fat planes within musculature is a very reassuring sign that FDG avidity is probably physiologic.

As with the skeleton, FDG PET helps visualize metastases that may be occult or overlooked on anatomic imaging. Muscle is an uncommon site for metastasis; therefore it is an organ that may not be scrutinized by the radiologist on every scan. FDG avidity highlights potentially important findings for additional scrutiny ( Fig. 4.4 ).

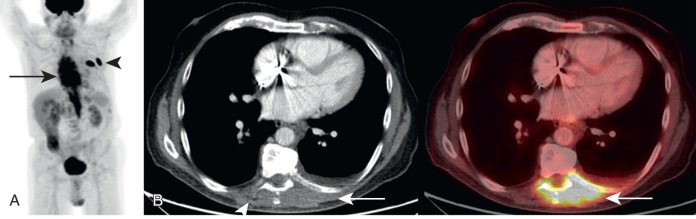
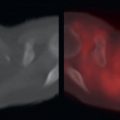
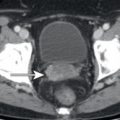
Unfortunately, as with other organ systems, FDG avidity could lead to the misinterpretation of benign findings. Focal areas of physiologic muscular FDG avidity could be mistaken for FDG-avid lymph nodes or other suspicious FDG-avid lesions. One area of muscle for which mistakes may occur is the crura of the diaphragm. The diaphragmatic crura may appear to have focal FDG avidity on individual axial slices, and this may be confused with retrocrural or upper abdominal lymph nodes ( Fig. 4.5 ). Similarly, not all histologies of malignancy will be readily apparent on FDG PET, and the corresponding CT images may demonstrate an abnormality within the muscle better than the FDG PET images. For example, myxoid tumors will demonstrate low attenuation compared to skeletal muscle, and muscular metastases from myxoid tumors may be more readily apparent on the CT component of the PET/CT ( Fig. 4.6 ).


Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


