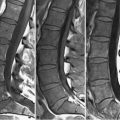
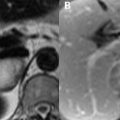
95 Musculoskeletal Neoplasms The distinction between benign and malignant bone tumors is frequently not possible on MRI, although benign lesions generally possess well-defined peripheral margins and lack adjacent soft tissue masses and spare cortical bone. The high SI of cartilage on T2WI aids in the identification of chondroid lesions. Osteochondromas are the most common benign osseous tumor, the cortex of these lesions being continuous with the parent bone. A hyperintense (on T2WI) cartilaginous cap greater than 1.5 cm in thickness in the presence of a closed physis suggests chondrosarcomatous degeneration as do low SI foci—correlating with calcification—therein. A surrounding dark rim of perichondrium may be visualized on T2WI. Enchondromas may also degenerate into chondrosarcomas—indicated by adjacent soft tissue, epiphyseal, or cortical invasion— although those outside the appendicular long bones and axial skeleton tend to be benign. Lobules of chondroid matrix distinguish such lesions from a bone infarction. The classic fluid-fluid level of an aneurysmal bone cyst involving the talus is illustrated on FS T2WI (A) and T1WI (B) of Fig. 95.1. The fluid-fluid level is a result of differences in densities and MRI SI appearances of cystic fluid contents, relating to the stage of blood products within. This finding is also associated with telangiectatic osteosarcoma, but can be seen in other entities as well, including giant cell tumors. A fluid-fluid level is present on the sagittal T2WI of the lumbar spine in Fig. 95.1C. Here, it is associated with an expansile, enhancing osteoblastoma arising from the right vertebral pedicle on the contrast-enhanced T1WI of Fig. 95.1D
![]()
Stay updated, free articles. Join our Telegram channel



Full access? Get Clinical Tree


