and Linh T. Ho3
(1)
Kaiser Permanente, Southern California Permanente Medical Group, Riverside, CA, USA
(2)
Molecular Imaging Center and PET Clinic, University of Southern California, Los Angeles, CA, USA
(3)
Department of Radiology, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
Case 10.1: Primary Osseous Lymphoma

History
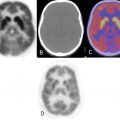
Patient is a 27-year-old woman with left proximal tibial lesion. Recent MRI showed aggressive mass like marrow replacement throughout the proximal right tibia with cortical thinning and disruption. PET-CT is requested as part of initial staging.
Findings
There is an intensely active left proximal tibial lesion extending approximately 11 cm from the tibial plateau inferiorly with mixed lytic sclerotic changes on CT, predominantly sclerotic, and maximum SUV up to 27.5 (Fig. 10.1). Other smaller hypermetabolic satellite foci are seen within the left proximal tibia. This lesion was subsequently biopsied and consistent with diffuse large B-cell lymphoma. The patient had received chemotherapy followed by radiation treatment.

Fig. 10.1
Impression
Local disease in the left proximal tibia
No other active in the remaining body
Pearls and Pitfalls
FDG PET-CT can detect other disease sites and shows the most active area which is useful for biopsy planning.
Primary osseous lymphoma can mimic other bone tumors.
Discussion
Primary lymphoma of the bone is a rare malignant condition that accounts for less than 5 % of all primary bone tumors. The vast majority of cases are of the non-Hodgkin type, with Hodgkin disease accounting for 6 % of cases. It is rare for patients younger than 10 years and occurs slightly more often in males. The femur is the most common site (especially in the metadiaphysis) and is affected in 25 % of cases. Other sites include the pelvis, humerus, head and neck, and tibia. Distinguishing primary bone lymphoma from other bone tumors is important because the former has a better response to therapy and a better prognosis (Fig. 10.1).
Case 10.2: Extra-Adrenal Paraganglioma

History
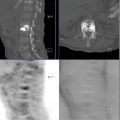
Patient is a 38-year-old female with newly diagnosed paraganglioma of the lower lumbar spine and upper sacrum.
Findings
There is an intensely active 4.5 × 7.8 × 5.6 cm soft tissue mass (maximum SUV of 8.9) centered in the lower lumbar and upper sacral spinal canal from the level of L4 through S2–3 (Fig. 10.2). This mass demonstrates osseous involvement of the L5, S1, and S2 vertebral bodies and posterior elements, consistent with the documented paraganglioma.

Fig. 10.2
Impressions
Hypermetabolic soft tissue mass centered in the lower lumbar and upper sacral spinal canal, consistent with the known paraganglioma
No definite evidence of distant metastasis
Pearls and Pitfalls
FDG PET positivity is almost a constant feature of pheochromocytomas and paragangliomas.
Whole-body PET-CT study is helpful in detecting distant metastases.
Discussion
Pheochromocytomas and extra-adrenal paragangliomas are rare tumors of neuroectodermal origin. They belong to the heterogeneous family of neuroendocrine tumors. Pheochromocytomas and paragangliomas show consistent 18F-FDG avidity, with maximum SUV ranging from 1.9 to 42 in nonmetastatic tumors and 2.3–29.3 in metastatic tumors. FDG PET is superior to 131I-metaiodobenzylguanidine in the majority of metastatic patients (Fig. 10.2).
Case 10.3: Low-Grade Fibromyxoid Sarcoma

History
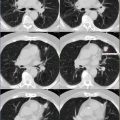
Patient is a 77-year-old man presented with left thigh mass. He is being seen for staging.
Findings
There is a moderately active 5.7 × 10.5 × 15 cm left distal thigh mass with maximum SUV of 4.6, consistent with neoplasm (Fig. 10.3). The mass has mixed areas of increased and decreased metabolic activity. The patient subsequently had biopsy which was consistent with low-grade fibromyxoid sarcoma.

Fig. 10.3
Impression
Heterogeneous hypermetabolic soft tissue mass in the left distal thigh, consistent with neoplasm
No definite evidence of distant metastasis
Pearls and Pitfalls
Whole-body PET-CT study is helpful in detecting distant metastases.
PET-CT is useful in biopsy planning to show the most metabolically active area of the tumor.
More accurate staging with FDG PET can help guide and ensure the most appropriate therapy.
Discussion
Low-grade fibromyxoid sarcoma is a rare soft tissue neoplasm with a bland histologic appearance that nevertheless can follow an aggressive course with multiple local recurrences and eventual metastasis to the lung and sometimes bone (Fig. 10.3).
Case 10.4: Elastofibroma Dorsi

History
Patient is a 73-year-old female with history of bilateral breast carcinoma, status post bilateral mastectomies. She is being seen for restaging.
Findings
Moderately active soft tissue densities are seen in bilateral subscapular regions, with maximum SUV of 3.7 on the right and 3.1 on the left (Fig. 10.4). These masses are located just deep relative to the serratus anterior muscles, displacing the muscle laterally. The soft tissue masses are oblong in shape, being longest in the superior-inferior plane. The attenuation of the lesions is similar to that of muscle, consistent with elastofibroma dorsi (EFD).

Fig. 10.4
Impressions
Bilateral EFD
No definite evidence of recurrent or metastatic disease
Pearls and Pitfalls
The diagnosis of EFD is made on the basis of the typical subscapular location of the lesions and the characteristic CT appearance (poorly circumscribed soft tissue with attenuation similar to that of muscle).
EFD also shows hypermetabolism on FDG PET.
Discussion
Elastofibromas are benign, slowly growing lesions characteristically located in the subscapular region. Elastofibromas are pseudotumorous lesions characterized by fibroblastic proliferation and accumulation of abnormal elastic fibers. They are relatively common lesions; the prevalence revealed on CT was found to be 2 %, and an autopsy series reported an 11–24 % prevalence. A lack of awareness of the CT characteristics of EFD could have resulted in erroneous interpretation of the PET portion of the studies. The FDG hypermetabolism may have been attributed to an inflammatory or neoplastic process (Fig. 10.4).
Case 10.5: Fibrous Dysplasia

History
Patient is a 38-year-old female with history of breast cancer. She is being seen for restaging.
Findings
Expansile cortex with ground-glass appearance of the right posterior seventh rib, with associated moderate activity (maximum SUV of 3.4), consistent with fibrous dysplasia (FD) (Fig. 10.5).