CHAPTER 66 Myocarditis
Definition
Myocarditis refers to focal or diffuse inflammation of the cardiac muscle associated with myocyte damage or necrosis and lymphocyte infiltration as a result of various infectious, immune, or nonimmune insults in the absence of significant acute or chronic ischemia.1–3
Prevalence and Epidemiology
Myocarditis is found in 1% to 10% of postmortem examinations; however, the true prevalence is unknown because of its insidious and variable clinical presentation.1,2 It accounts for 20% of cardiac causes of sudden deaths in military recruits1 and 40% of acute presentations of dilated cardiomyopathy.2 Up to 50% of patients with acquired immunodeficiency syndrome (AIDS) have evidence of myocarditis on biopsy.2
Etiology and Pathophysiology
Infections are a major cause of myocarditis. Viruses, such as coxsackieviruses A and B and other enteroviruses, adenovirus, influenza virus, and Epstein-Barr virus, are the most important causes of myocarditis in the United States.2,4 A wide range of bacteria (Streptococcus, Chlamydia, Neisseria, Borrelia) and parasites (Trypanosoma, Toxoplasma, Trichinella) can also cause myocarditis. Various medications, such as doxorubicin (Adriamycin) and sulfonamides, and toxins, such as cocaine, have also been associated with myocarditis. Large-vessel vasculitis, such as Takayasu arteritis, and autoimmune diseases, such as systemic lupus erythematosus, sarcoidosis, and Wegener granulomatosis, are also important but rare causes of myocarditis.2,4
Manifestations of Disease
Clinical Presentation
The clinical manifestation of myocarditis is variable, ranging from progressive dyspnea and weakness to left ventricular failure to sudden death. Patients may present with influenza-like symptoms, such as fever, fatigue, malaise, and arthralgia.1–3 Arrhythmia is common.4 In addition, chest pain with abnormal electrocardiographic (ECG) recordings and serum troponin elevation in patients with myocarditis can mimic acute myocardial infarction.5 Patients may also present at a late stage with dilated cardiomyopathy.4
Imaging Indications and Algorithm
Imaging plays a pivotal role in the diagnosis of myocarditis. In the past, endomyocardial biopsy was once considered the gold standard for diagnosis of myocarditis; however, it has been shown to have low sensitivity due to sampling error related to the patchy nature of the disease.6 Echocardiography and cardiac MRI should be part of the initial diagnostic evaluation in conjunction with ECG and serum troponin evaluation. More selected biopsy, if needed, may be performed with the MRI result as a guide.5 Coronary computed tomographic angiography (CTA) can be performed in the acute setting to exclude significant coronary arterial stenosis in patients with myocarditis who are presenting with chest pain, raised abnormal cardiac enzymes, and abnormal ECG changes.
Imaging Technique and Findings
Radiography
Chest radiographs may be completely normal in patients with myocarditis, especially acutely (Fig. 66-1). Alternatively, cardiomegaly, interstitial or alveolar pulmonary edema, pleural effusions, and pericardial effusion may be detected as a result of left ventricular failure.2 Less commonly, right ventricular failure may be manifested by right atrial enlargement, prominent azygos vein, and superior vena cava enlargement.
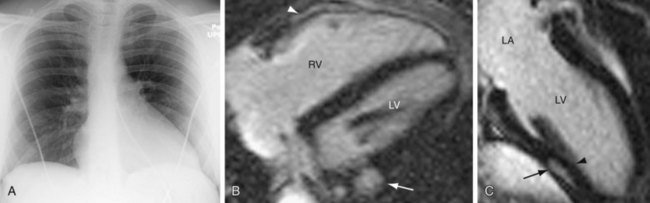
 FIGURE 66-1
FIGURE 66-1Ultrasonography
Echocardiographic findings of myocarditis are nonspecific, including segmental wall motion abnormalities and increased left ventricular volume.7 During the acute phase, transient left ventricular wall thickening can be observed, probably related to interstitial edema.8,9 The average brightness of the myocardium is also higher in patients with myocarditis than in control patients.10
Computed Tomography
On delayed enhanced images, nodular, patchy, bandlike enhancement of the mid and epicardial layer of the left ventricular wall can be seen in patients with myocarditis (Fig. 66-2).11 In a study of 12 consecutive patients with acute chest pain consistent with myocardial ischemia and normal coronary angiogram, delayed enhanced MDCT performed 5 minutes after injection of contrast material demonstrated the same accuracy as MRI in differentiating between myocardial infarction and myocarditis in the acute phase.12 Similarly, another study also showed good correlation in the extent and location of hyperenhancement at MDCT compared with cardiac MRI in the early phase of suspected acute myocarditis.13

 FIGURE 66-2
FIGURE 66-2


