Fig. 1
Mucinous cystic neoplasm. (a–c) Surgical specimen (distal pancreatectomy): pancreatic huge neoplasm (a) in the body-tail of the pancreas presenting as a cystic mass (b); the cavity is lined by a mucinous epithelium (c) with typical subepithelial ovarian-like stroma (asterisks in c) (Courtesy of Piccin Editore, Milan, Italy)
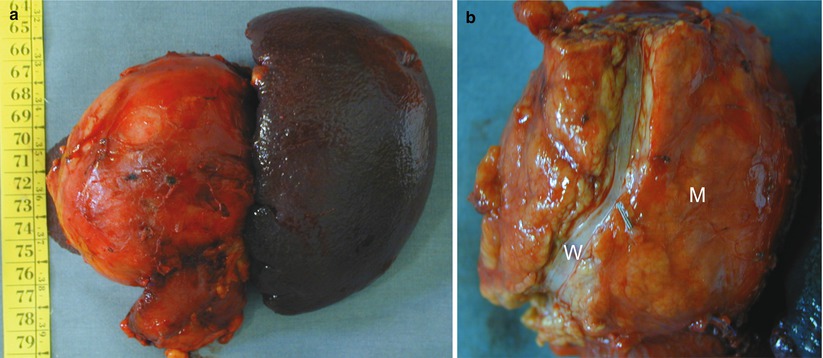
Fig. 2
Mucinous cystic neoplasm. (a, b) Surgical specimen (distal pancreatectomy): pancreatic neoplasm (a) in the tail of the pancreas presenting as a cystic mass. The lesion does not communicate with the Wirsung duct in fact no fluid leakage from the mass (M in b) is present after longitudinal cut of the main pancreatic duct (W in b)
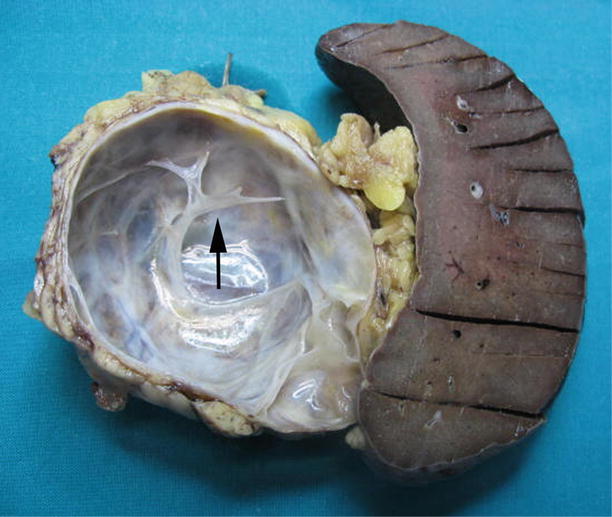
Fig. 3
Mucinous cystic neoplasm. Surgical specimen (distal pancreatectomy): pancreatic mucinous cystic neoplasm presenting as a cystic mass with few intralesional septa (arrow)
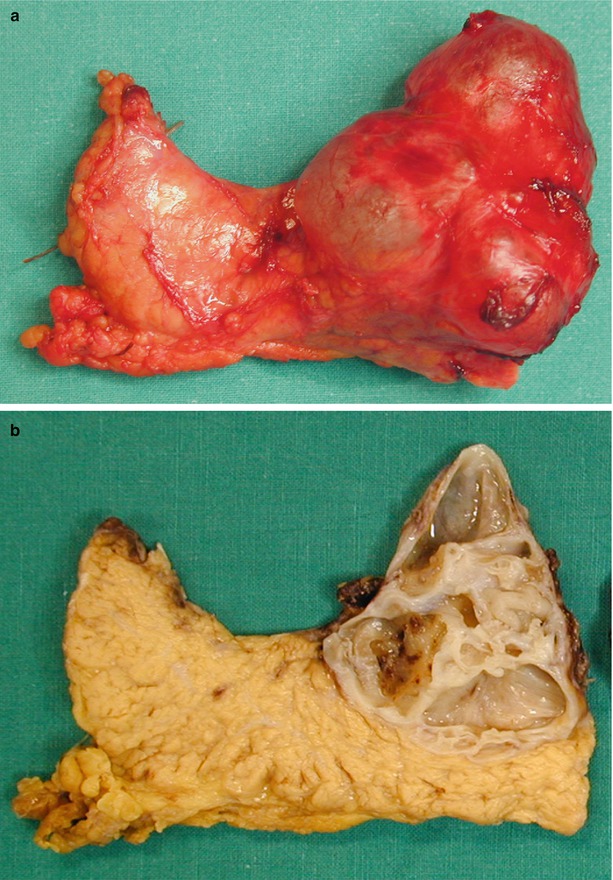
Fig. 4
Mucinous cystic neoplasm. (a, b) Surgical specimen (distal pancreatectomy): pancreatic neoplasm presenting as a cystic mass (a) with numerous intralesional septa shown in the cut section (b)

Fig. 5
Multiloculated mucinous cystic neoplasm. Surgical specimen (distal pancreatectomy): pancreatic mucinous cystic neoplasm presenting as a cystic mass with multiple intralesional septa, delineating multiple locules along the internal wall
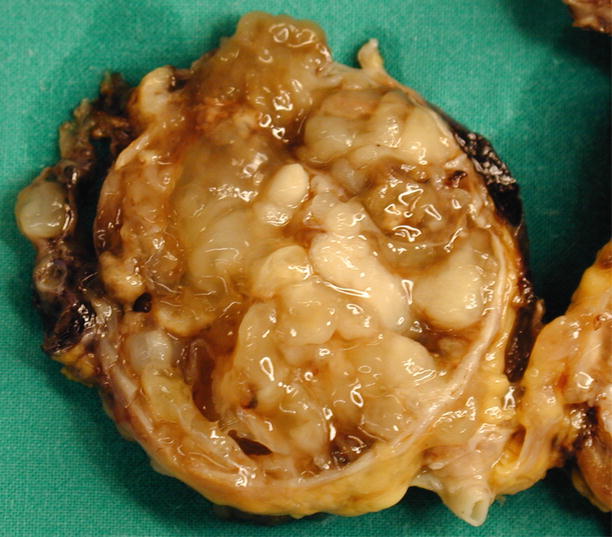
Fig. 6
Complex mucinous cystic neoplasm. Surgical specimen (distal pancreatectomy): pancreatic mucinous cystic neoplasm presenting as a complex cystic neoplasm with irregular thick wall and filled by thick tenacious mucoid material (Courtesy of Piccin Editore, Milan, Italy)
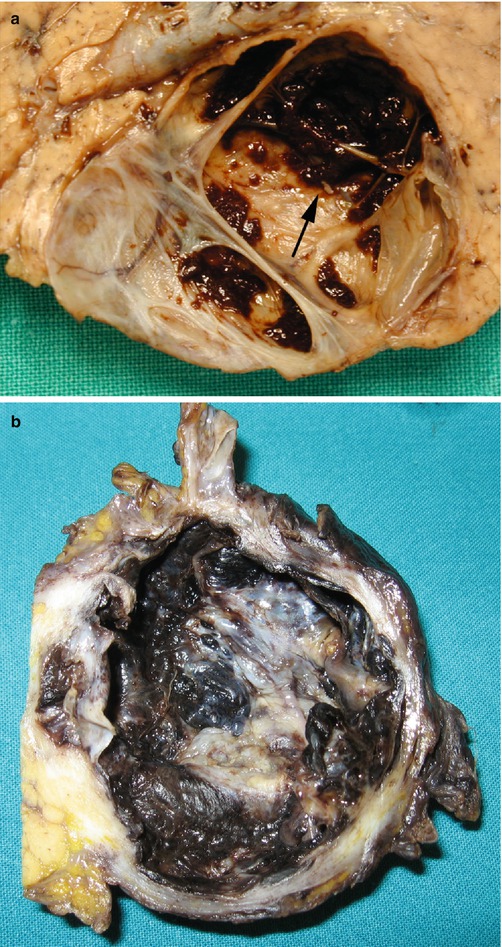
Fig. 7
De-epithelized mucinous cystic neoplasm. (a) Surgical specimen (distal pancreatectomy): pancreatic mucinous cystic neoplasm presenting as a cystic mass with few intralesional septa and focal de-epithelized internal wall (arrow), appearing as a brown area on the cut section. (b) Surgical specimen (distal pancreatectomy): pancreatic mucinous cystic neoplasm presenting as a cystic unilocular mass with amply de-epithelized internal wall, appearing as diffuse brown areas on the cut section, resembling a pseudocyst
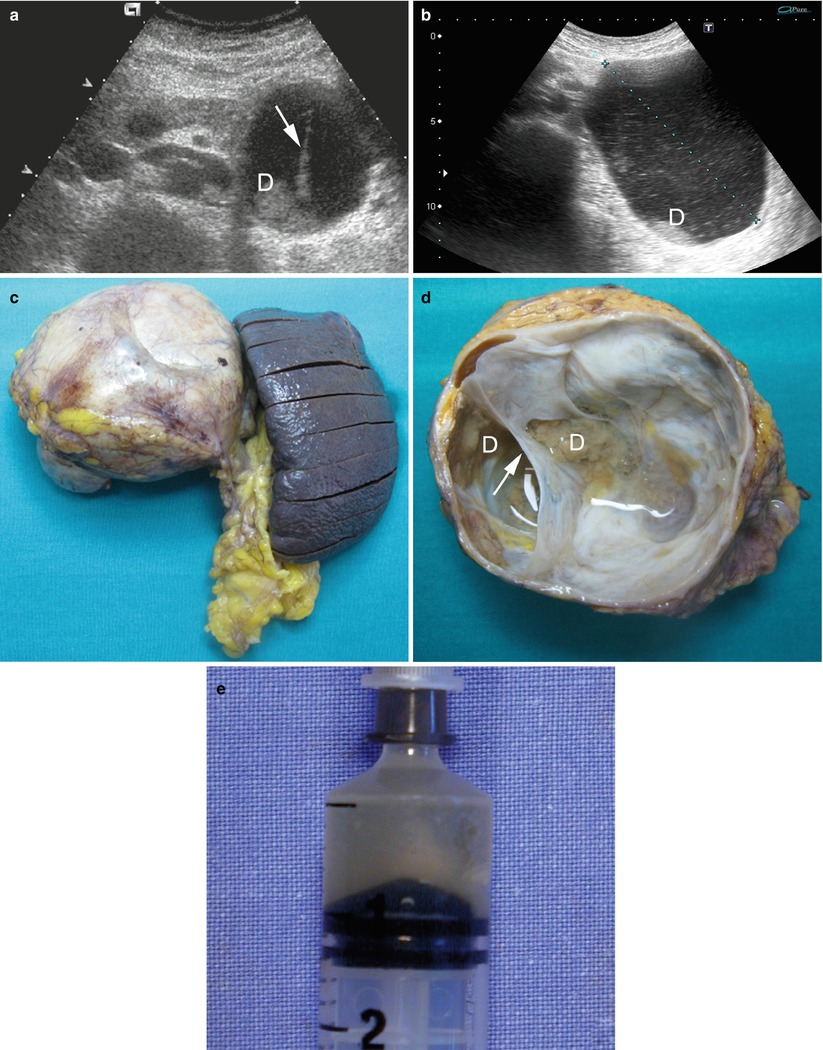
Fig. 8
Mucinous cystic neoplasm. (a) Ultrasound study: cystic mass of the pancreatic body with thick wall, intracystic septa (arrow) and echoic deposit (D). (b) Ultrasound study: huge cystic mass (calipers) of the pancreatic body with cystic corpuscular content and echoic deposit (D). (c) Surgical specimen (distal pancreatectomy): pancreatic huge neoplasm in the body-tail of the pancreas. (d) On the cut section the neoplasm is cystic with thin septa (arrow) and deposits (D). (e) Cystic fluid: after the aspiration the intracystic fluid is typical torpid and opaque
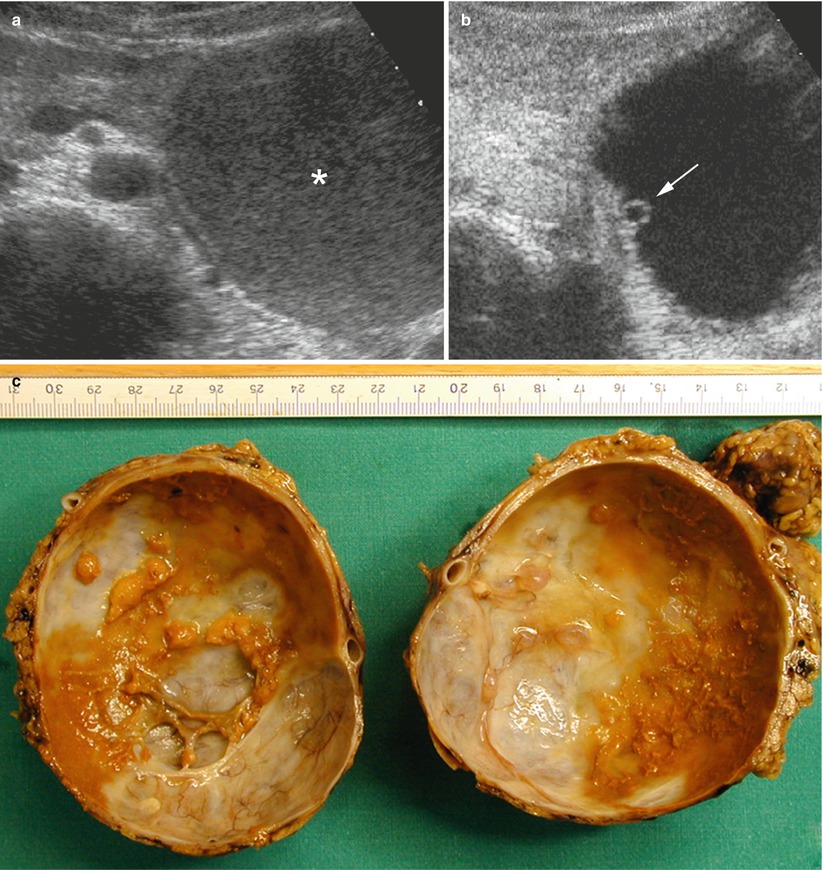
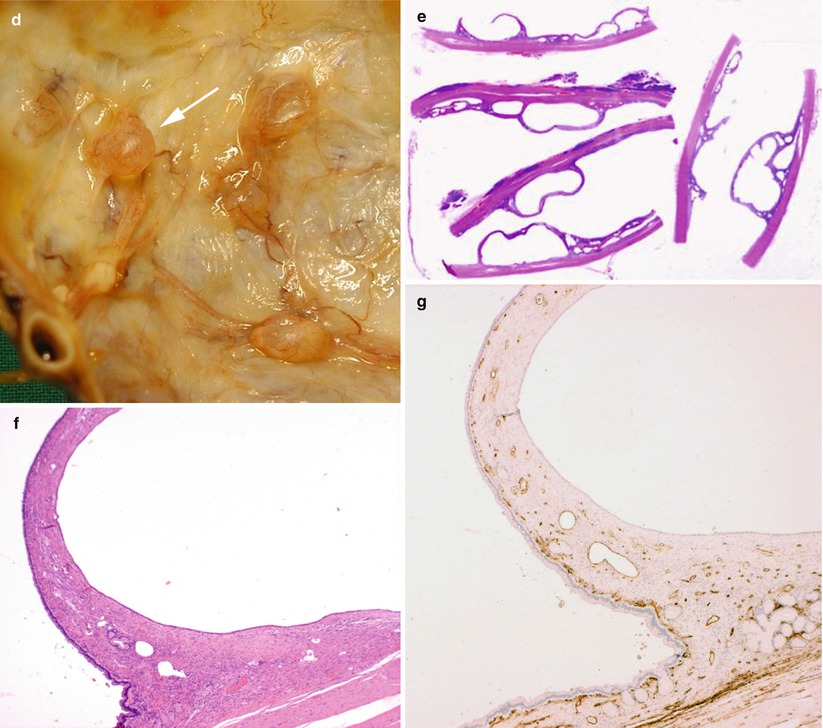
Fig. 9
Mucinous cystic neoplasm. (a, b) Ultrasound study: cystic mass in the pancreatic body with corpuscular content (asterisk in a). Only at CEUS (b), a small vascularized septum along intracystic wall (arrow in b) is visible. (c–g) Surgical specimen (distal pancreatectomy) and histopathology: mucinous cystic neoplasm with thick wall and small septa, delineating small locules along the internal wall at cut section (c). The small septa are better visible on the detail image (arrow in d). Histological image (e) of small septa along the wall. Detail histological image of small septum at hematoxylin–eosin stain (f), showing mucinous epithelium with subepithelial ovarian-like stroma. Along the small septum, multiple tiny vessels are marked (brown trace) on CD34 stain (g) (Courtesy of Piccin Editore, Milan, Italy)
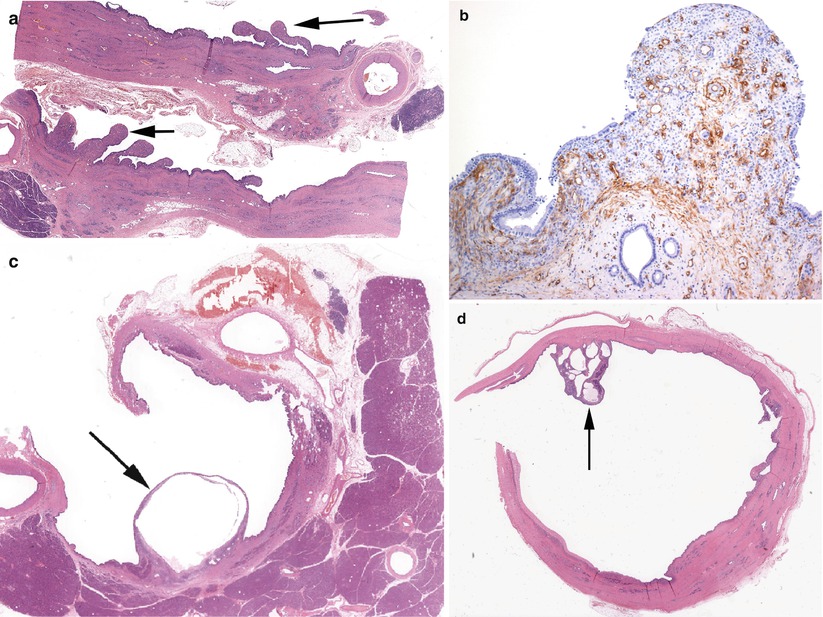
Fig. 10
Mucinous cystic neoplasm internal wall. (a, b) Histopathology: mucinous cystic neoplasm with thick wall and irregular internal surface with trabecular projections (arrows in a) in which, at CD34 immunohistochemical stain (b), multiple thin vessels (brown trace in b) are visible. (c) Histopathology: mucinous cystic neoplasm with thin septum (arrow) delineating an internal cystic locule along the wall. (d) Histopathology: mucinous cystic neoplasm with internal vegetation (arrow) along the internal wall, characterized by a cluster of irregular septa delimiting small cysts
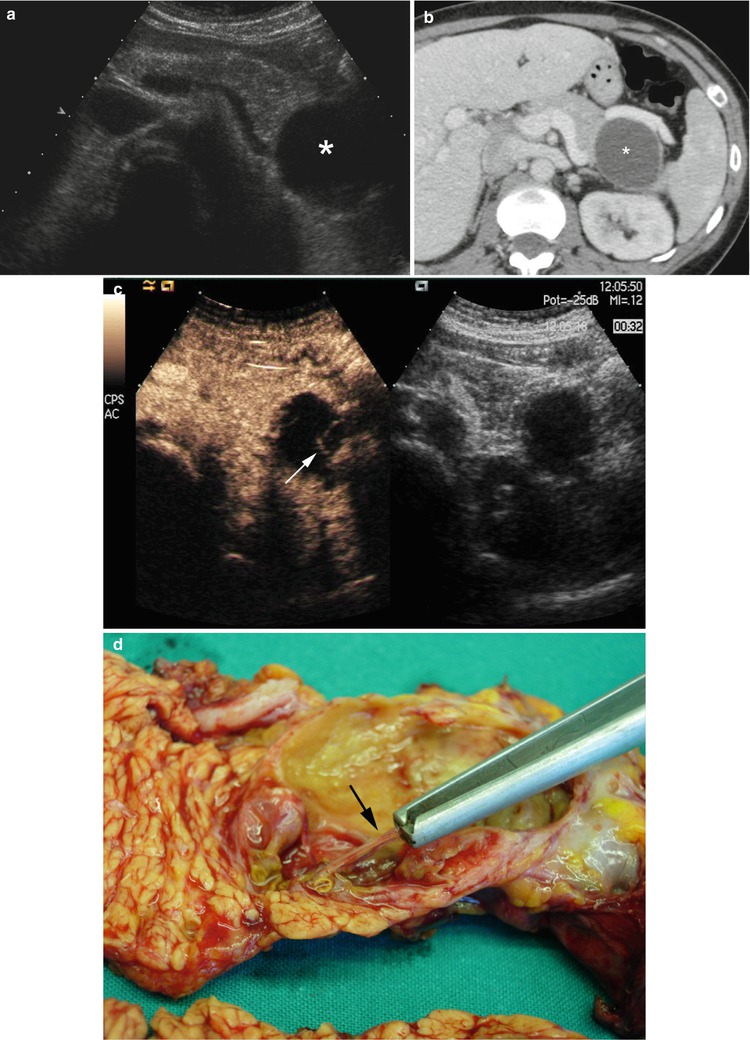
Fig. 11
Mucinous cystic neoplasm. (a) Ultrasound study: incidental cystic lesion (asterisk) in the pancreatic body. (b) CT study: the cystic lesion (asterisk) is confirmed in the pancreatic body; no septa are detected within the lesion. (c) CEUS: after contrast medium injection thin septa (arrow) in the cystic lesion are clearly visible. (d) Surgical specimen (distal pancreatectomy): thin intralesional septa (arrow) are confirmed on the cut section
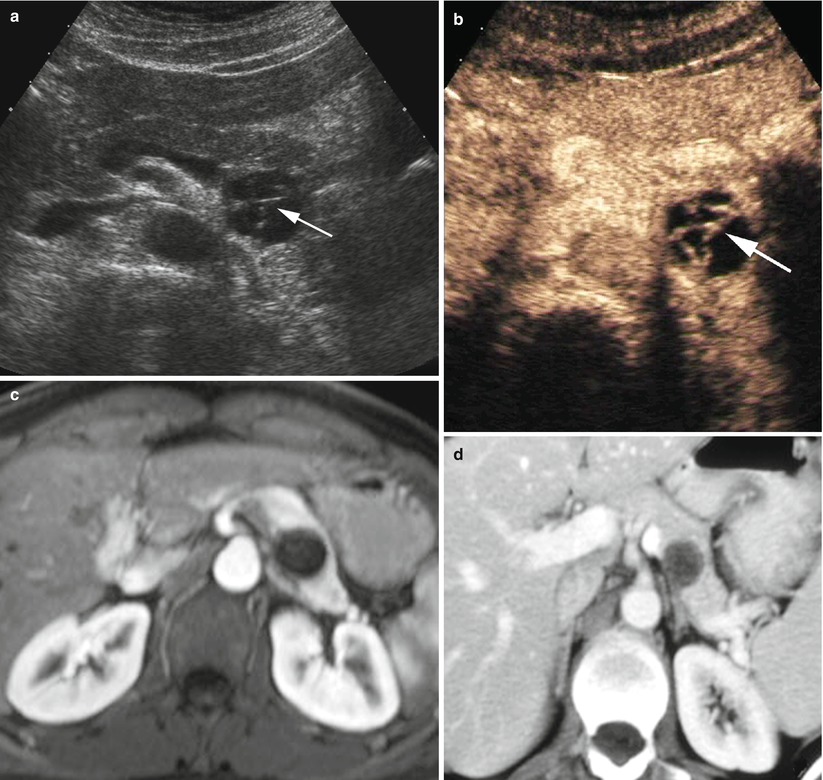
Fig. 12
Mucinous cystic neoplasm. (a, b) Ultrasound study: incidental small cystic lesion in the pancreatic body-tail with thin intracystic septa visible at ultrasound (arrow in a) and vascularized at CEUS (arrow in b). (c, d) MRI and CT studies: both dynamic MRI (c) and CT (d) did not provide the same detailed representation of septa
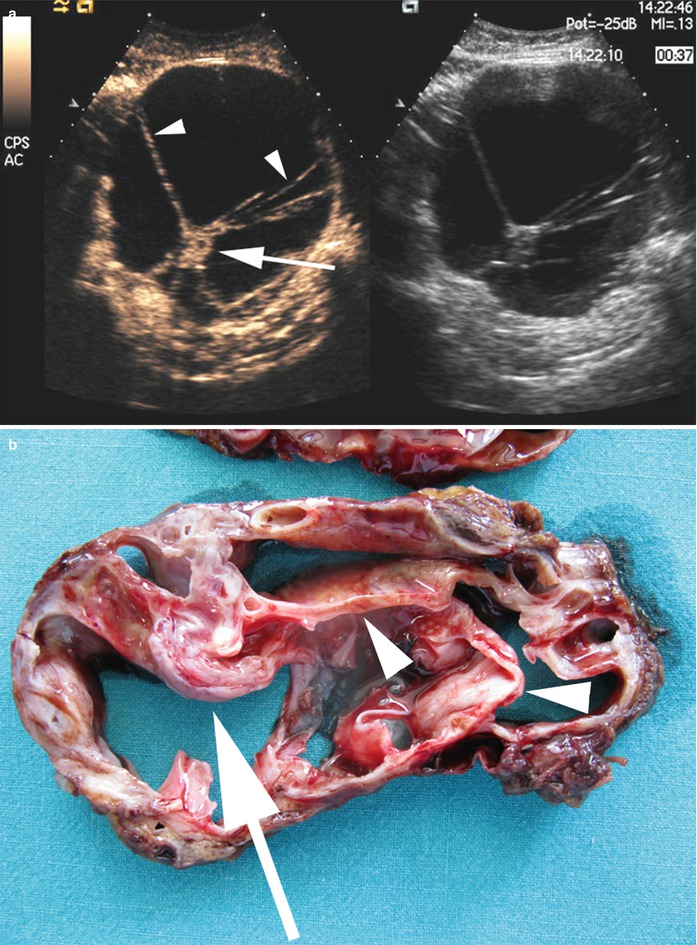
Fig. 13
Mucinous cystic neoplasm and pathological correlation. (a) CEUS: cystic mass with several vascularized septa (arrowheads) and enhancing nodule (arrow). (b) Surgical specimen: septa (arrowheads) and nodule (arrow) are confirmed
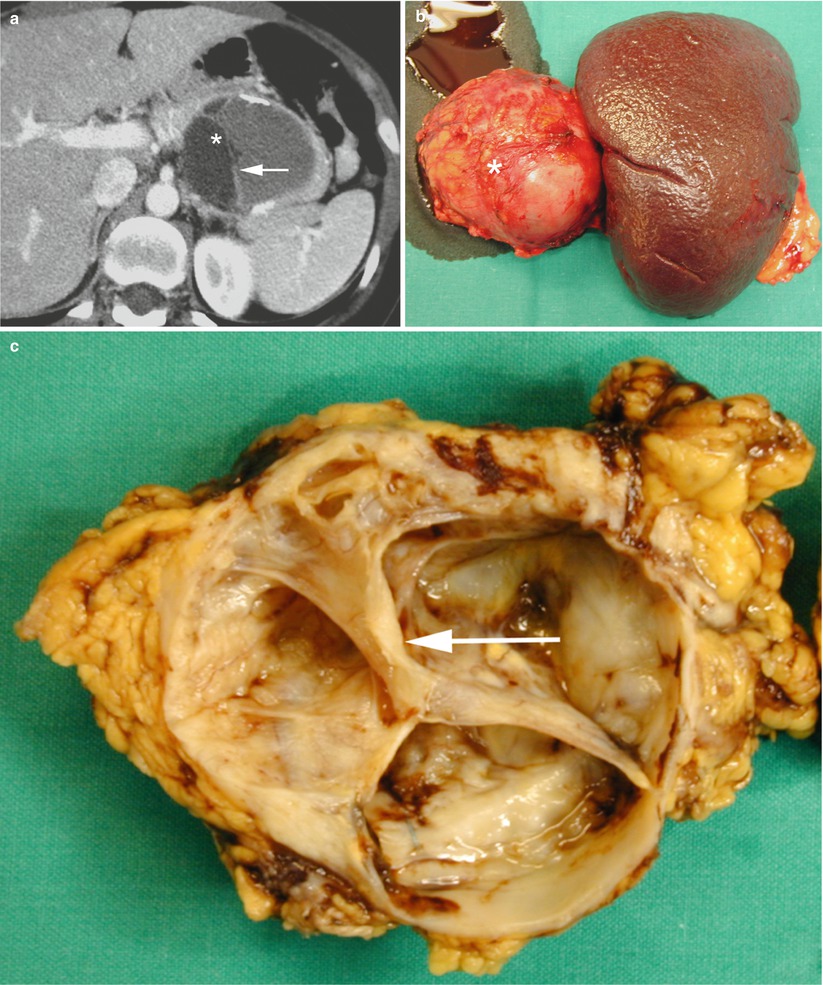
Fig. 14
Mucinous cystic neoplasm with septa. (a) CT study: cystic mass (asterisk) with thick wall, containing lamellar calcifications, and septa (arrow). (b, c) Surgical specimen (distal pancreatectomy) of different case: mucinous cystic neoplasm appearing as a cystic mass (asterisk in b) with thick septa (arrow in c) on cut section
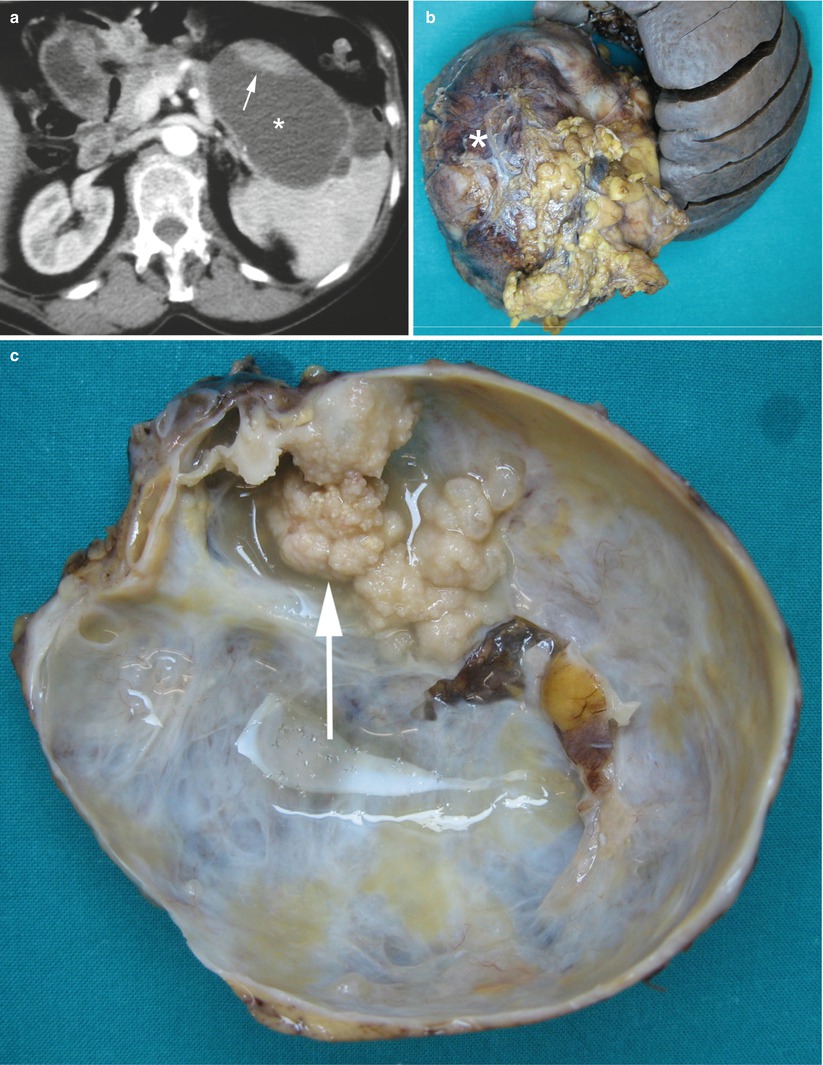
Fig. 15
Mucinous cystic neoplasm with nodule. (a) CT study: huge cystic mass (asterisk) with thick wall and nodule (arrow) hyperdense on dynamic phase. (b, c) Surgical specimen (distal pancreatectomy) of different case: huge mucinous cystic neoplasm appearing as a cystic mass (asterisk in b) with septa and nodular solid projections (arrow in c) on cut section
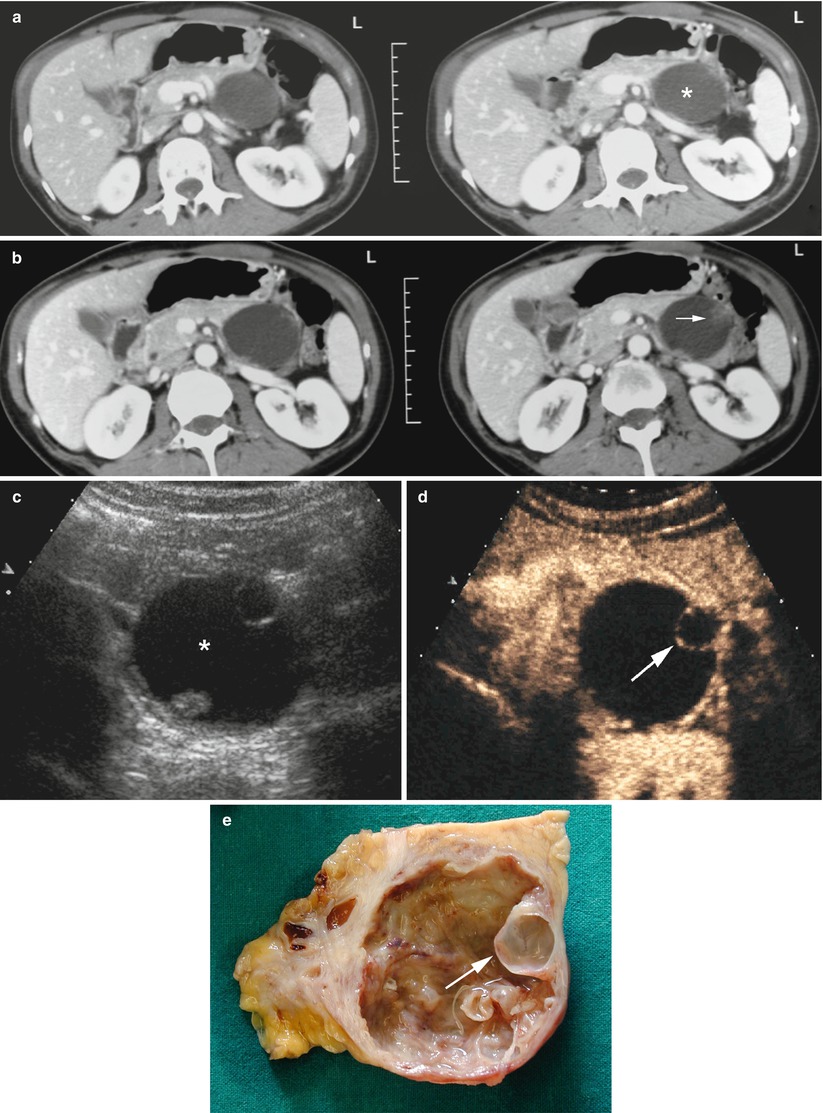
Fig. 16
Mucinous cystic neoplasm and pathological correlation. (a, b) CT study: cystic mass (asterisk in a) with unclear vegetations (arrow in b) hyperdense in the dynamic phase. (c, d) CEUS: cystic mass (asterisk in c) with well-detailed septa (arrow in d) vascularized in the dynamic phase. (e) Surgical specimen (distal pancreatectomy): mucinous cystic neoplasm with septa (arrow) delineating small cystic locule along the internal wall on cut section
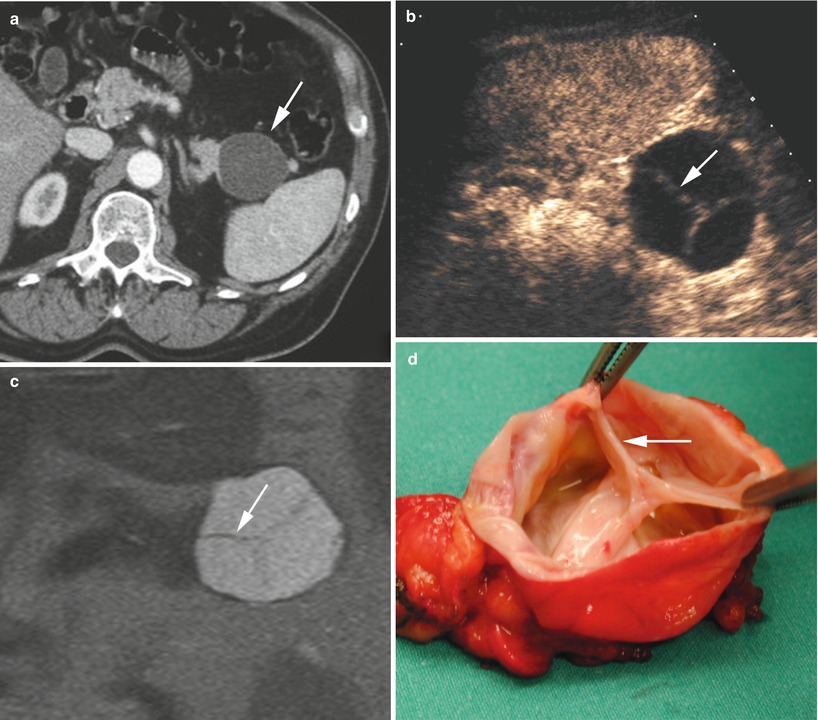
Fig. 17
Mucinous cystic neoplasm and pathological correlation. (a) CT: small cystic mass (arrow) completely hypodense without any septa. (b) CEUS: small cystic mass with well-detailed vascularized septa (arrow). (c) MRI: small cystic mass with well-detailed septa (arrow). (d) Surgical specimen (distal pancreatectomy): mucinous cystic neoplasm with septa (arrow) dividing the cavity in three locules on cut section
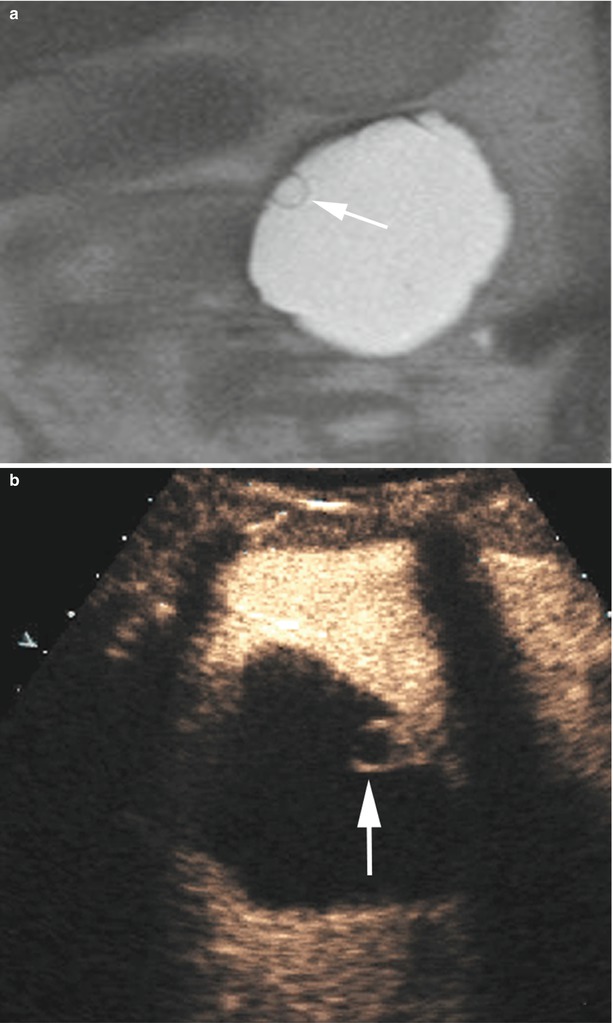
Fig. 18
Mucinous cystic neoplasm and imaging correlation. (a) MRI: cystic mass with very small well-detailed septum (arrow). (b) CEUS: cystic mass with very small well-detailed vascularized septum (arrow)
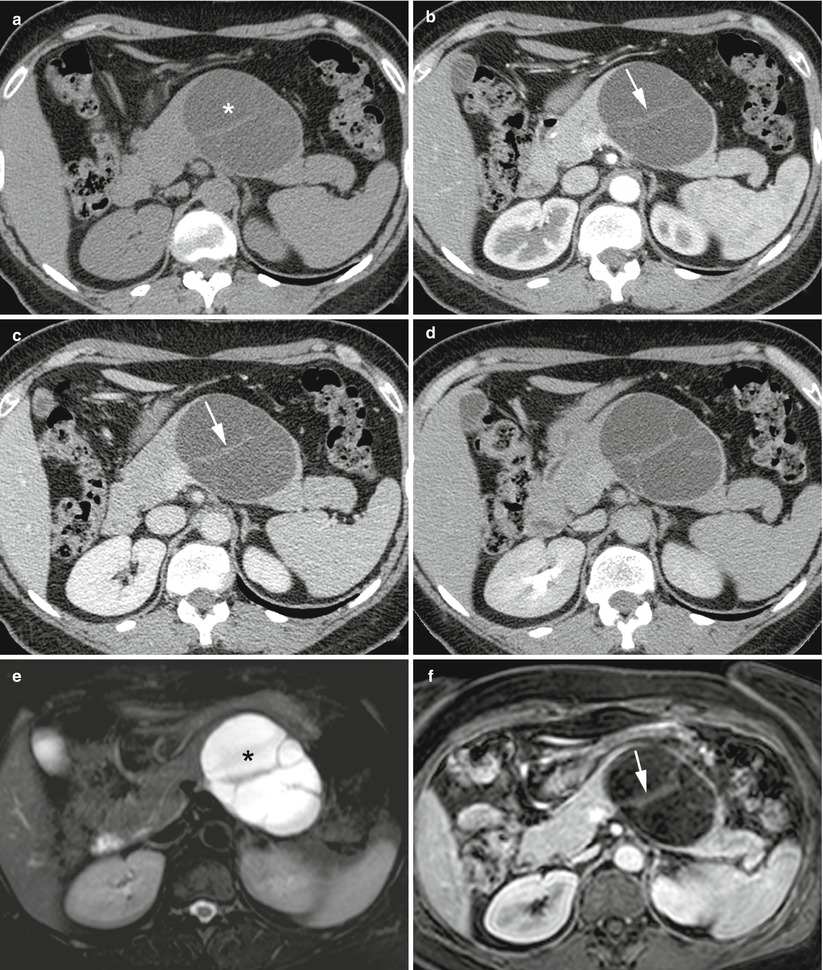
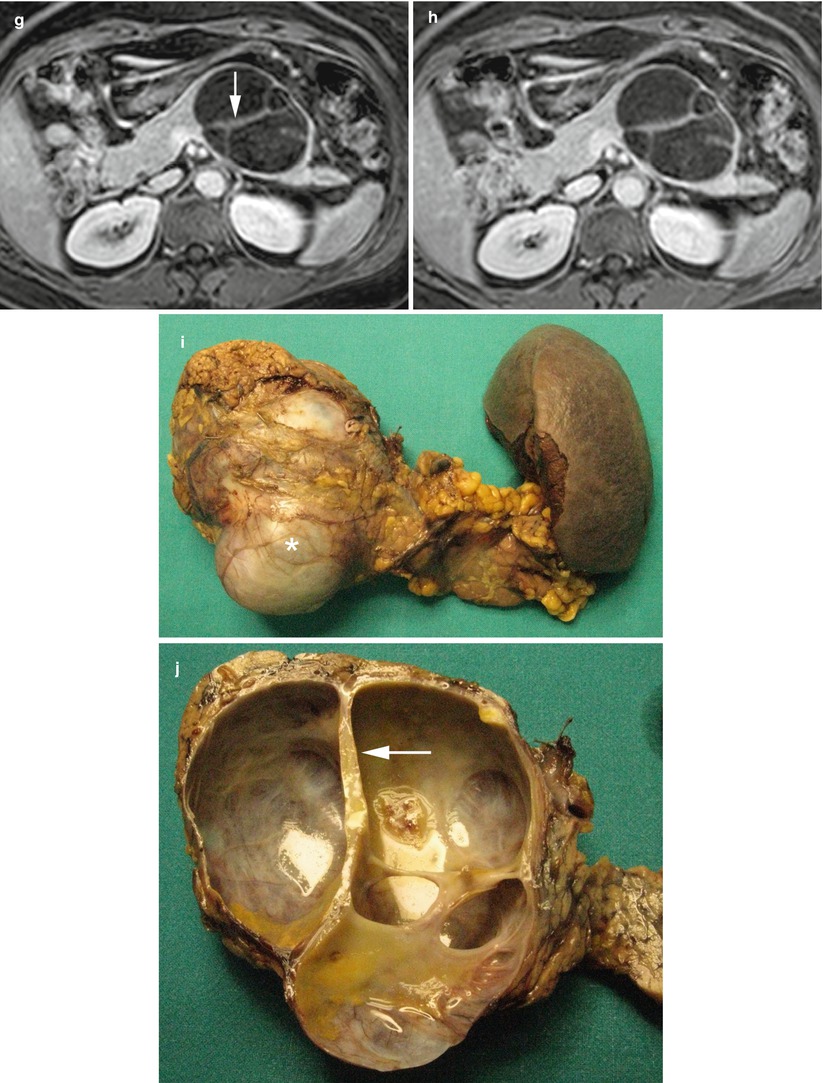
Fig. 19




Imaging and pathological correlation of mucinous cystic neoplasm. (a–d) CT study: large cystic mass in the pancreatic body appearing hypodense (asterisk in a) in the baseline scan with thick wall and septa (arrow in b and c) well visible in the pancreatic (b), venous (c), and late (d) dynamic phases. (e–h) MRI study: large cystic mass in the pancreatic body appearing hyperintense (asterisk in e) on T2-weighted fat-saturated images showing thick wall and enhancing septa (arrow in f and g) in the pancreatic (f), venous (g), and late (h) dynamic phases. (i, j ) Surgical specimen (distal pancreatectomy): large neoplasm in the body of the pancreas appearing as a cystic mass (asterisk in i) with thick wall and thick septa (arrow in j) on cut section
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
