The article summarizes classification schemes of spinal trauma and rules to decide on proper imaging modality after a spinal trauma. High-risk factors that recommend imaging are, for instance, age 65 years or older, a dangerous trauma mechanism, and paresthesia in the extremities. More recent classification schemes include evaluation of the posterior ligamentous complex, for which MR imaging is the best modality, and to give therapeutic recommendations for conservative or surgical management. MR imaging is the imaging method of choice when spinal cord injury, cord compression, or ligamentous injury is suspected. MR imaging is the method of choice to depict epidural or intramedullary hemorrhage and sequelae of spinal trauma.
Key points
- •
In the absence of high-risk factors as defined, for instance, by the Canadian C-Spine Rule (CCR) in alert and stable trauma patients, no imaging is necessary at all.
- •
MR imaging is the imaging method of choice, when spinal cord injury, cord compression, or ligamentous injury is suspected, especially in obtunded patients.
- •
Direct injury of the spinal cord may result in ischemia, edema, and hemorrhage and MR imaging can detect these changes already in the hyperacute und acute stages.
- •
The incidence of posttraumatic syringomyelia increases with time period after the injury.
Epidemiology of spinal trauma
The rate of spinal trauma shows wide international variation. According to systemic reviews of international studies, the incidence and mortality of spinal column and spinal cord injuries are significantly higher in developing compared with developed countries. For instance, in the United States, the incidence of traumatic spinal cord injury in 2010 was approximately 40 per million per year, or approximately 12,400 annually. A bimodal age distribution is demonstrated in most studies, with a first peak in adolescents and young adults between 15 and 29 years of age and a second peak in adults older than 65 years of age. The mortality is significantly higher in older patients. Spinal trauma is more common in men. In descending order, motor vehicle accidents, falls, violence, and sport accidents are the most common causes of spinal cord injuries. The exposed localization and the higher degree of mobility between the head and torso predispose the cervical spine to injuries, in particular, the vertebrae around the craniocervical and cervicothoracal junction. The ribcage leads to more rigidity and stability of the thoracal spine compared with the thoracolumbar junction. Thus, spinal injuries are most often located in the cervical spine, followed by the thoracolumbar junction.
Epidemiology of spinal trauma
The rate of spinal trauma shows wide international variation. According to systemic reviews of international studies, the incidence and mortality of spinal column and spinal cord injuries are significantly higher in developing compared with developed countries. For instance, in the United States, the incidence of traumatic spinal cord injury in 2010 was approximately 40 per million per year, or approximately 12,400 annually. A bimodal age distribution is demonstrated in most studies, with a first peak in adolescents and young adults between 15 and 29 years of age and a second peak in adults older than 65 years of age. The mortality is significantly higher in older patients. Spinal trauma is more common in men. In descending order, motor vehicle accidents, falls, violence, and sport accidents are the most common causes of spinal cord injuries. The exposed localization and the higher degree of mobility between the head and torso predispose the cervical spine to injuries, in particular, the vertebrae around the craniocervical and cervicothoracal junction. The ribcage leads to more rigidity and stability of the thoracal spine compared with the thoracolumbar junction. Thus, spinal injuries are most often located in the cervical spine, followed by the thoracolumbar junction.
Indications for imaging of the traumatic spine
In the United States, each year many trauma patients at risk for spine injury are treated in emergency departments, but only a small percentage of these patients have a spine fracture. To enhance the efficiency, sensitivity, and specificity of the utilization of radiologic examinations, and thus save resources, approved clinical decision tools or rules should be consulted to determine if a radiologic examination is reasonable. These clinical decision rules consider variables from the patient history and examination or simple clinical tests, were derived from clinical research, and are defined as decision-making tools. The most established clinical decision rules for spinal imaging are the CCR and the National Emergency X-Radiography Utilization Study Low-Risk Criteria (NLC) ( Table 1 ). By identifying high-risk criteria ( Box 1 ), both clinical decision tools help if radiography is indicated as a screening method on alert (eg, score of 15 on the Glasgow Coma Scale) and stable trauma patients with mild or unspecific symptoms and low risk of spine injury. In the absence of high-risk factors in alert and stable trauma patients, no imaging is necessary at all. When high risk-factors are identified in these patients, however, imaging is suggested.
| National Emergency X-Radiography Utilization Study Low-Risk Criteria | Low-Risk Canadian C-Spine Rule |
|---|---|
|
|
High-risk criteria of CCR
Age greater than 65 years
Dangerous mechanism (ie, high-speed motor vehicle accident or fall from heights over 1m)
Paresthesia in extremities
Further high-risk criteria
Altered mental status
Multiple fractures
Drowning or diving accidents
Significant head or facial injury
Rigid spinal disease (ie, ankylosing spondylitis, diffuse idiopathic skeletal hyperostosis)
A large prospective multicenter cohort study in 9 Canadian emergency departments, comparing the CCR and NLC in trauma patients in stable condition, showed that the CCR has a significantly higher sensitivity and specificity for cervical spine injury than the NLC, and that its consequent use would result in reduced rates of radiography. Therefore, the CCR is visualized as standard operating procedure in Fig. 1 and is used as reference at the authors’ institution.
In the acute phase of the injury period, flexion-extension radiography is not useful, because of muscle spasm, and dynamic fluoroscopy should not be used to evaluate for ligamentous injury in obtunded patients.
In patients with high-risk criteria, multiple sites of trauma, correlating neurologic deficits or trauma mechanisms proposing an injury of the spine, imaging of the spine with computed tomography (CT) and if necessary, and not contraindicated, MR imaging is indicated. Among the advantages of CT is its widespread availability. Also, due to multidetector CT technology, CT needs a short time of image acquisition and CT has the potential of diagnostic evaluation of adjacent organs within the scanned body region. Moreover, CT yields an unsurpassed contrast of osseous structures. The radiation dose of a CT scan has to be considered, especially in young patients, and when scanning the pelvis and lumbar spine. Due to its superior soft tissue contrast, MR imaging is the method of choice for visualizing neural tissue, intervertebral disks, and ligamentous structures. Nevertheless, an immediate MR imaging examination may be not possible in every emergency department, and the contraindications (eg, most cardiac pacemakers or other electrically stimulating implants and loose metallic objects), the long duration of the examination, and the potentially limited possibilities of patient monitoring during the MR imaging examination have to be taken into account. No contraindications assumed, an immediate MR imaging after spinal trauma is indicated when CT or neurologic symptoms suggest an injury of neural, or ligamentous structures and when an adequate neurologic examination cannot be performed, even when the CT scan turned out to be normal.
The American College of Radiology Appropriateness Criteria for Suspected Spine Trauma summarizes several conclusions. No imaging should be performed in patients with positive low-risk criteria by NLC or CCR. In adults with high-risk criteria by NLC or CCR, multidetector CT (with multiplanar reformatting) is the recommended imaging method. Once a decision for imaging is made, the entire spine should be examined, considering the high incidence of noncontiguous multiple injuries. Thoracic and lumbar CT examinations can be derived from thoracic-abdomen-pelvis CT, instead of primary scanning of the spine. In children up to 14 years, radiography is the imaging method of choice: recommended views for cervical spine are anterior-posterior, lateral, and open mouth. Recommended views for thoracic and lumbar spine are anterior-posterior and lateral. Because radiography has a limited diagnostic use in adults, it should be used primarily for resolving nondiagnostic CT scans due to motion artifacts. In the acute injury period, flexion-extension radiography is not useful, due to muscle spasm. MR imaging is the imaging method of choice, when spinal cord injury, cord compression, and/or ligamentous injury is suspected, especially in obtunded patients. Dynamic fluoroscopy should not be used for evaluation of ligamentous injury in obtunded patients.
Radiologic classifications of spinal trauma
Traditional Classification Schemes Based on Fracture Localization and Morphology
Traditional classification schemes of spinal fractures are exclusively based on description of the location and morphology of the fracture. Thus, CT or even plain radiography is sufficient for using these classifications.
Craniocervical junction
Occipital condyle fractures
Anderson and Montesano classified condyle fractures in 3 categories ( Fig. 2 ): type I, impacted fracture of the occipital condyle; type II, basilar skull fracture, including an occipital condyle fracture; and type III, displaced avulsion fracture on the occipital condyle. Types I and II are supposed to be stable, whereas type III is unstable, due to potentially associated tear of alar ligaments.
Atlas fractures
The classification of fractures of the atlas, according to Gehweiler and colleagues, differentiates 5 types: type I, fracture of the anterior arch; type II, fracture of the posterior arch; type III, combined fracture of anterior and posterior arch, so-called Jefferson fracture; type IV, fracture of lateral mass; and type V, fracture of transverse process ( Fig. 3 ). Fractures of the atlas can be associated with injuries of the vertebral artery, in particular in type V fractures, indicating CT or MR angiography.
Odontoid fractures
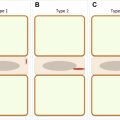
According to Anderson and d’Alonzo, fractures of the odontoid process of the axis are classified in 3 types: type I, avulsion of the odontoid tip; type II, fracture of odontoid body; and type III, basilar fracture of the axis ( Fig. 4 ). Although originally considered stable, the stability of type I fractures is discussed controversially, because of the avulsion of the apical odontoid ligament. Type II fractures are unstable, whereas most type III fractures are supposed to be stable.
Axis fractures
Fractures of the axis with traumatic spondylolysis can be classified according to Effendi and colleagues in 3 types: type I, isolated nondisplaced fracture; type II, traumatic spondylolisthesis with greater than or equal to 3-mm anterior displacement of C2 on C3 and disruption of C2/C3 disk; and type III, traumatic spondylolisthesis with disruption of C2/C3 disk and disruption of facet joints ( Fig. 5 ). In fractures of the axis, the vertebral artery is at risk for injuries. In cases of axis fractures, an associated injury of the vertebral artery should be excluded by CT or MR angiography.
Thoracolumbar fractures
Fractures of the thoracolumbar spine can be classified according to the 3-column model of Denis. The anterior column includes the anterior longitudinal ligament and the anterior two-thirds of the vertebral body and intervertebral disk. The middle column includes the posterior third of the vertebral body and intervertebral disk and the posterior ligament. The posterior column includes spinous process, ligamentum flava, and the interspinous, supraspinous, and intertransverse ligaments ( Fig. 6 ). Injuries of more than 1 column are unstable. Isolated injuries of the middle column are not possible. Usually, impaction fractures affect the anterior and middle column; flexion-distraction injuries affect the anterior and posterior column.
The most accepted and comprehensive classification of thoracal and lumbar spine fractures is based on Magerl and was adopted by the AO Foundation. The trauma mechanism is classified as A (impaction), B (distraction), and C (rotation) ( Fig. 7 ). To accommodate the variety and complexity of possible fractures, each of these 3 main categories can be categorized in subgroups. A0, minor, nonstructural fractures; A1, wedge-compression fractures; A2, split fractures; A3, incomplete burst fractures; A4, complete burst fractures; B1, posterior band disruption; B2, distraction of the posterior arch (Chance fracture), B3, hyperextension; C, multidirectional with translation, displacement, or dislocation. Although established for thoracolumbar fractures, in clinical routine, this classification is often used for injuries of the cervical spine as well.