Spinal infection is rare. Clinical suspicion is important in patients with nonmechanical neck and/or back pain to make the proper diagnosis in early disease. Before planning surgery, a thorough evaluation of the spinal stability, alignment, and deformity is necessary. Timing of surgery, side of approach, appropriate surgical technique, and spinal instruments used are crucial. Biomechanical preservation of the spinal column during and after the infection is a significant issue. Postoperative spine infection is another entity of which spinal surgeons should be aware of. Proper septic conditions with meticulous planning of surgery are essential for successful spine surgery and better outcome.
Key points
- •
Spinal infections may be life threatening.
- •
Surgery is indicated in inadequate biopsies, conservative treatment failure, neurologic deterioration, spinal instability and deformity.
- •
In abrupt neurologic deterioration, emergency surgery must be performed.
- •
Choice of the operative procedure depends on the causative agent, site of the lesion, neurologic status, and bone destruction.
Introduction
Spinal infections are rare pathologies that compromise 2% to 4% of all bone infections. These infections often jeopardize both the integrity of the spinal column and its neural contents, creating a consumptive process that may be life threatening. Therefore, in recent years more attention has been paid to spinal infections with the availability of increased diagnostic accuracy. Yet, even with improved diagnostic tools and procedures, delays in diagnosis remains an important issue. Spinal infections can be categorized according to the different entities, such as contagious agent, anatomic localization, and onset of disease. There is usually also a predisposing factor that compromises the immune system and affects the spread as well as the severity of disease. Postoperative spinal infections are an important topic. Management of spinal infections requires a multidisciplinary approach involving spinal surgeons, infectious disease specialists, radiologists, rehabilitation personnel, psychologists, and social services. We emphasize neurosurgical approaches to spinal infections, focusing on anatomic location and causative agent.
Normal anatomy
Spinal infections are located mainly in the epidural space, body of the vertebra, intervertebral disc, perivertebral area, and intradural space. Infection may be localized in one of these compartments. Erosion of vertebral endplates causes deformation of the cortical lining and spreads to disc space (spondylodiscitis), subligamentous paravertebral space (paravertebral and psoas abscesses), and/or epidural–intradural space (epidural abscesses, intradural abscesses, and meningitis), consecutively.
Introduction
Spinal infections are rare pathologies that compromise 2% to 4% of all bone infections. These infections often jeopardize both the integrity of the spinal column and its neural contents, creating a consumptive process that may be life threatening. Therefore, in recent years more attention has been paid to spinal infections with the availability of increased diagnostic accuracy. Yet, even with improved diagnostic tools and procedures, delays in diagnosis remains an important issue. Spinal infections can be categorized according to the different entities, such as contagious agent, anatomic localization, and onset of disease. There is usually also a predisposing factor that compromises the immune system and affects the spread as well as the severity of disease. Postoperative spinal infections are an important topic. Management of spinal infections requires a multidisciplinary approach involving spinal surgeons, infectious disease specialists, radiologists, rehabilitation personnel, psychologists, and social services. We emphasize neurosurgical approaches to spinal infections, focusing on anatomic location and causative agent.
Normal anatomy
Spinal infections are located mainly in the epidural space, body of the vertebra, intervertebral disc, perivertebral area, and intradural space. Infection may be localized in one of these compartments. Erosion of vertebral endplates causes deformation of the cortical lining and spreads to disc space (spondylodiscitis), subligamentous paravertebral space (paravertebral and psoas abscesses), and/or epidural–intradural space (epidural abscesses, intradural abscesses, and meningitis), consecutively.
Pathology
The spine is known to be susceptible to infections with the incidence varies between 1:100,000 and 1:250,000 in developed countries. According to the literature, mortality rate ranges between 2% and 17%. There is a superiority in males and age distribution has 2 peaks: under age 20 and between age 50 and 70.
The major causative agents of spine infections are bacteria, which cause pyogenic infections; tuberculosis (TB) or fungi, which are responsible for granulomatous infections; and parasites, which are the least common etiology. Among them, the majority are bacterial pyogenic infections owing to Staphylococcus aureus . Of note, in one-third of all cases of spinal infections, the infectious agent could not be identified.
Pathogen spread occurs via 3 routes: hematogenous, direct external inoculation (iatrogenic), and spread from contiguous tissues. Risk factors for spinal infections include previous spine surgery, distant infectious foci, diabetes mellitus, malnutrition, advanced age, intravenous drug abuse, human immunodeficiency virus infection, a history of malignancy, prolonged use of steroids, rheumatologic disease, liver cirrhosis, renal failure, and septicemia. Among these, previous spine surgery is most common (30%), without regard to the operative technique.
Management
Management can vary according to the type of the causative agent, localization of the disease, neurologic condition, general status of the patient, and stability as well as alignment of the spinal column. The most frequently affected spinal segments are lumbar (58%), thoracic (30%), and cervical (11%). Clinical signs and symptoms caused by spinal infections often are subtle and insidious; therefore, clinical suspicion in patients with nonmechanical pain is important in making a proper diagnosis in early stage of the disease.
Diagnostic studies must be targeted toward anatomic segments of the disease, anatomic localization of the infection, neurologic status of the patient, clinical onset of the disease, the structure of the spine, and the causative agent ( Table 1 ). In many cases, the causative agent is inferred; therefore, the empirical treatment is given. After or even all diagnostic tools are used, biopsy is recommended for the analysis of the organisms.
| Anatomic Segments | Anatomic Localization | Neurologic Status | Clinical Onset | Structure of Spine | Causative Agent |
|---|---|---|---|---|---|
| Cervical (upper) | Vertebral body | Intact | Acute | Alignment (No/Ne/K) | Pyogenic |
| Cervical (subaxial) | Intervertebral disc | Neurologic deficit | Subacute | Stability (S or Uns) | Fungal |
| Thoracic | VB + ID | Chronic | Destruction | Parasitic | |
| Lumbar | Epidural | Others | |||
| Sacral | Subdural | ||||
| Multisegmental | Intamedullary | ||||
| Paravertebral |
Biopsy
Closed (Percutaneous) Biopsy
The rate of definite diagnosis is 68% to 86%. Percutaneous CT-guided needle biopsy is found to be safe and its accuracy has been reported up to 70%. Recently, endoscopic biopsy is used in cases of spondylodiscitis, because it also allows discectomy and drainage, and its performance for bacterial recovery is better than CT-guided spinal biopsy. The paramedian Kambin triangle for sampling of the intervertebral disc is the primary approach. The Kambin’s triangle is defined as a right triangle over the dorsolateral disc. The hypotenuse is the exiting nerve root, the base (width) is the superior border of the caudal vertebra and the height is the dura/traversing nerve root. The transpedicular approach is another route that is defined for the percutaneous biopsies.
Open Biopsy
Patients who have already received antibiotic therapy can have false-negative biopsy results. If the first biopsy is negative, a second biopsy should be done after an antibiotic-free duration of time. If the second biopsy is also negative, then open surgical biopsy should be considered. Overall, 30% of biopsies are sterile. Open biopsy is indicated for cases with absolute indications to surgery and negative consecutive biopsy results. It is more accurate, and radical debridement is also possible.
Surgery
The timing of the surgery is directly related to neurologic status of the patient. Indications for surgery in spinal infections are listed in Box 1 . A broad range of options for the surgical management of spinal infections that can be chosen according to the pathology, patient status, and structure of the spine include anterior, posterior, combined, and minimally invasive approaches. The choice of the approach is related most closely to the presence of neurologic deficits, the location of the infection, and the degree of associated osseous destruction. The key principles for successful surgical treatment are summarized in Box 2 . Biomechanical preservation of the spine after infection is crucial for the follow-up period. Before planning the surgery, a thorough evaluation of the spinal stability, alignment, and deformity should be undertaken.
- •
Biopsy in false-negative biopsy cases
- •
Neurologic deficit
- •
Septicemia
- •
Instability
- •
Extensive bone destruction
- •
Deformity
- •
Intracanal lesion with mass effect
- •
Unknown etiologies associated with active mass lesion
- •
Failure of conservative treatment
- •
To diagnose undetermined cases if closed needle biopsy is insufficient;
- •
To debride the necrotic tissue for increasing the efficiency of the antimicrobial treatment
- •
To decompress the neural elements and to stabilize the spine in the setting of instability.
Pyogenic infections
Pyogenic Vertebral Osteomyelitis
Vertebral osteomyelitis and discitis account for 1% to 7% of all bone infections. These bacterial infections often hazard both the integrity of the spinal column and its neural contents. Lumbar lesions with nerve root deficits are usually benign, and the final outcome is satisfactory with and without surgery. However, compression of the thecal sac requires immediate operative intervention. Although upper cervical osteomyelitis is rare, it requires fusion because of the increased risk of instability.
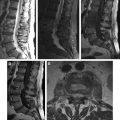
Generally, vertebral bodies and disc spaces are involved in pyogenic vertebral osteomyelitis, so the anterior approach is accepted as the standard method because it provides effective decompression and debridement. Laminectomy is contraindicated in such cases. Radical debridement at the spine comprises resection of the entire infected or necrotic disc and bony tissue, followed by anterior column reconstruction and placement of a strut graft that harvested from iliac bone or titanium cage, as well as a supplemental posterior instrumentation. Fusion is recommended in the appropriate conditions ( Fig. 1 ). Titanium mesh cages are stated to be as effective as iliac autografts by means of fusion. The metallic implants must be titanium, and not stainless steel, because of bacterial film colonization. For 1 level or 2 levels of pyogenic vertebral osteomyelitis, anterior surgery may be enough; however, in cases of long levels, posterior stabilization must be performed. Recent publications demonstrate that anterior fixation after debridement and fusion provides better correction of deformity, shorter operative time, fewer postoperative complications, and earlier rehabilitation than posterior fusion. The intact posterior elements preserve the function of the lumbar spine and improve the quality of life in the postoperative period.
Pyogenic infections rarely affect the posterior elements. Posterior debridement and decompression with laminectomies and posterior fusion should be performed in such cases. Of note, laminectomies should be avoided unless there is a posterior epidural compression and/or infection of the posterior structures. Moreover, to prevent deformity, posterior instrumentation should be performed as far above and below the infected levels as possible; bypassing the infected area may be suitable for some patients during medical therapy. A favorable outcome by controlling the infection and reconstruction of the spinal segment can generally be obtained by medical and/or surgical treatment. Delay in diagnosis and inadequate therapy lead to mortality.
Pyogenic Spondylodiscitis
A needle biopsy sample should be obtained via fluoroscopy, or with CT-guided intervention. Recently endoscopic techniques are used in cases of spondylodiscitis, because they allow discectomy and drainage and their performance for bacterial recovery is better. Initially conservative treatment with immobilization and antibiotics in cases with minor destruction or minimally invasive abscess reduction, for example, epidural catheters with local antibiotic instillation aiming at a spontaneous fusion of the vertebral bodies or at least fibrous stiffness. However, in some cases, radical surgery with debridement, autologous bone grafting, and stabilization with the possibility to correct deformities is recommended increasingly.
Minimally invasive techniques have had their primary indication in less severe cases with small abscess and little bone destruction. Endoscopic interventions are also appropriate choices for debridement and irrigation, followed by percutaneous drainage. Moreover, percutaneous transpedicular discectomy and drainage are also applicable and result in immediate pain relief. The posterior approach is indicated in cases of an epidural abscess in the lumbar spine. Large epidural abscesses should be drained emergently because posterior migration of the abscess may result in paraplegia. Patients with multisegmental involvement or distinct substance loss are reported to benefit from a combined approach with ventral debridement and bony bridging, including additional dorsal stabilization.
Pyogenic Epidural Abscess
Most pyogenic epidural abscesses arise from adjacent spondylodiscitis that are often located in the anterior aspect of the spinal canal. Spinal epidural abscesses account for 0.2 to 2 cases per 10,000 hospital admissions. In addition to main surgical indications, epidural abscess even without associated neurologic deficits especially in the cervical and thoracic regions can also be considered as a necessity for operative intervention. Relative indications include uncontrolled pain and contraindications for conservative treatment. Percutaneous endoscopic lavage and drainage are the most recent techniques for diagnostic and therapeutic purposes. This technique is usually the choice for treatment in cases without neurologic deficits and instability. Recent publications have stated that this technique is also effective in multilevel abscesses and recurrent infections. The operative approach depends on the location of the infection. Anterior decompression is necessary for spinal epidural abscess located in the anterior segment of the epidural space; this intervention is usually combined with anterior corpectomy. Laminectomy, hemilaminectomy, or both should be performed for cases that are located posteriorly. Facet joints should be left intact to keep spinal stability and alignment intact after the operation. In children, laminatomy or laminaplasty is preferred because of an attempt to close the posterior covering of the spinal canal is tried after the surgical intervention. After temporary removal of the spinous processes and vertebral laminae, the spinous processes are reconnected to the roots of the vertebral arch of the corresponding vertebrae, once abscess drainage has been undertaken. In most of cases, minimal bone removal without affecting stability is sufficient; therefore, there is no need for additional fusion or stabilization. However, stabilization and fusion should be performed for unstable cases. Late diagnosis is associated with mortality.
Granulomatous infections
Tuberculosis
Spinal TB accounts for less than 1% of all TB cases; affected patients are at extremely high risk for neurologic deficits and severe spinal deformities. If the patient is intact neurologically and there is no evidence of spinal instability, treatment should be managed conservatively with chemotherapy and immobilization with a brace or corset. Surgical indications are same as for other spinal infections that are summarized in Box 1 . Additionally, the presence of kyphosis and instability owing to vertebral corpus destruction may also be considered. Surgical treatment offers an earlier fusion, quicker relief of pain, earlier return to previous activities, less bone loss, and therefore less kyphosis compared with conservative treatment.
Because the pathology is located typically in the vertebral bodies, debridement should be performed anteriorly. In addition, anterior debridement is essential in cases of neurologic impairment, multilevel involvement, or severe abscess formation. A thorough anterior approach consists of debridement of both the paraspinal abscess and the infected bone; decompression of the spinal canal with tricortical autogenous grafting combined by anterior internal fixation in 1 or 2 level spondylodiscitis should be performed ( Figs. 2 and 3 ). Anterior interbody fusion using a titanium mesh cage also provides solid fusion, maintenance of kyphosis correction, and no recurrence of infection in such patients. Also, it is well-known that infections of the cervical spine require surgical treatment more often when compared with other regions. In the setting of thoracic abscess in at most 2 levels without bony destructions and instability, thoracoscopic drainage is indicated.
Posterior approaches in TB should be the choice of intervention in limited cases that are restricted to posterior elements of the vertebral column and in the setting of a contraindication for anterior internal fixation. Posterior instrumentation and fusion procedures must also be added in cases that were laminectomized. In multilevel (>2 levels) disease, fixed kyphotic deformity, or in cases with a poor quality of adjacent bone strength, staged anterior and posterior intervention is recommended ( Fig. 4 ). Autogenous large fibular or tibial strut grafts are used for larger resection areas. In the setting of greater degrees of kyphotic deformity (>80° of kyphosis) and stiffer curves (25%> flexibility), several types of osteotomies may be helpful in both increasing the curve flexibility and to achieve a successful deformity correction. Being a less adhesive microorganism, Mycobacterium tuberculosis produces less ability to adhere the foreign substances, so colonization of metallic implants occurs only rarely. However, the use of stainless steel implants in vertebral osteomyelitis is not recommended. The correction of kyphosis should be performed if possible to create normal anatomic degrees, because it allows for more efficient stabilization and early mobilization, and is effective in the maintenance of correction achieved.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


