Placenta is a vital organ that connects the maternal and fetal circulations, allowing exchange of nutrients and gases between the two. In addition to the fetus, placenta is a key component to evaluate during any imaging performed during pregnancy. The most common disease processes involving the placenta include placenta accreta spectrum disorders and placental masses. Several systemic processes such as infection and fetal hydrops can too affect the placenta; however, their imaging features are nonspecific such as placental thickening, heterogeneity, and calcifications. Ultrasound is the first line of imaging during pregnancy, and MR imaging is reserved for problem solving, when there is need for higher anatomic resolution.
Key points
- •
Placenta is a vital organ connecting the maternal and fetal circulations.
- •
Placenta accreta spectrum disorders and placental masses are the most common indications for dedicated placental imaging with ultrasound or MR imaging.
- •
Placental accreta spectrum disorders present with characteristic imaging findings of irregular lakes, myometrial thinning, abnormal intraplacental vascularity, and placental bulge on ultrasound and MR imaging. Imaging is helpful in assessing the extent of involvement and presurgical planning.
- •
Antepartum hemorrhage is an important cause of maternal and fetal morbidity and mortality, and most of the cases are due to placenta abnormalities including placenta previa and placental abruption. MR imaging can help distinguish hematomas from other causes of antepartum bleeding, such as vasa previa, degenerated uterine fibroid, cervical pathology, and placental tumors.
- •
Placental masses are most commonly identified during the routine fetal ultrasound examinations. Imaging evaluation should focus on the effect of the mass on fetal well-being in this scenario.
Introduction
Placenta is a vital organ that allows exchange of nutrients and gases between the mother and the developing fetus. The placenta develops by 10 to 14 weeks of pregnancy and is fully functional by the end of the first trimester to support the hormonal needs of continuing the pregnancy and the metabolic needs of the developing fetus. As such, disease states that affect the placenta can have important consequences for both the mother and the fetus. ,
Ultrasound (US) is the first line of imaging for most placental diseases. Per guidelines, all pregnancies should have an “anatomy scan,” also called as a level one scan, at 18 to 20 weeks of gestation. Although most of this scan focuses on assessing the anatomic development of the fetus, evaluating the placenta is a crucial component of this examination. MR imaging has an increasingly important role as an adjunct modality for imaging for placental disease processes as well and can be particularly helpful for troubleshooting and advanced evaluation. ,
The most common placental pathologies for which imaging is necessary include placenta accreta spectrum disorders (PASD) and placental masses. Both processes are relatively uncommon; however, the adverse consequences to both the fetus and the mother are substantial and hence should be specifically sought after and never overlooked. This review addresses the normal anatomy of the placenta, imaging technique and protocols, imaging findings and summarizes the key information that needs to be conveyed to the clinical providers.
Normal anatomy and imaging technique
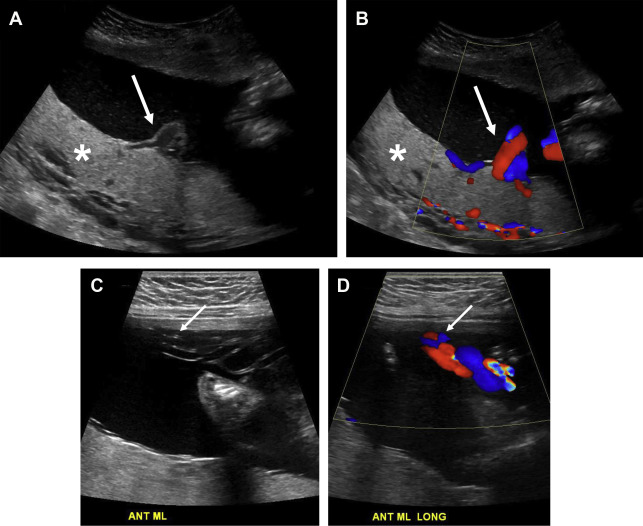
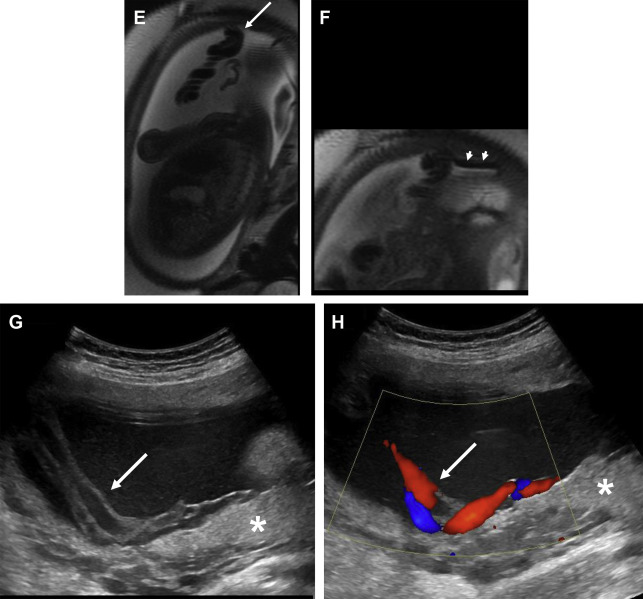
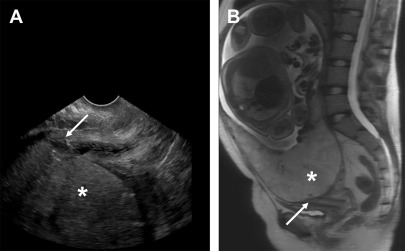
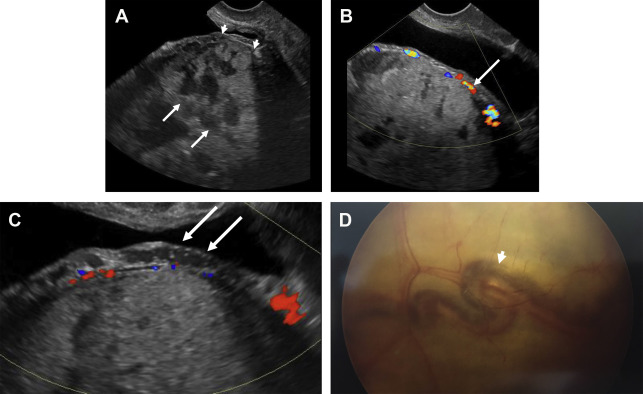
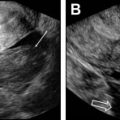
The normal placenta is a discoid structure with tapering edges, which attaches to the myometrium in a uniformly layering fashion. It measures up to 4 cm in maximum thickness. The umbilical cord mostly inserts centrally into the placenta but can be marginal or velamentous as well ( Fig. 1 ). Normally, the lower placental edge should be at least 2 cm from the margin of the internal cervical os. If less than 2 cm from the internal os, this counts as placenta previa. When the placenta covers the internal os, this constitutes complete previa ( Fig. 2 ). Sometimes, variant anatomy such as succenturiate lobe (portion of the placenta separate from the main placental mass) and vasa previa ( Fig. 3 ) are present, which are extremely important to detect and relay to the clinicians because of the risk of retention of this lobe during delivery and both conditions being at high risk for significant hemorrhage.
The normal placenta is homogeneous, slightly hyperechoic relative to the myometrium on grayscale US ( Fig. 4 ). On high-frequency and high-resolution images, the placenta may seem slightly less hyperechoic and overall the myometrium seems more closer in echogenicity to the placenta. Hence, this relative difference in echogenicity is based on sonographic technical parameters (see Fig. 4 ). Very few lakes may be present, especially adjacent to the placental cord insertion. On color Doppler imaging, few small caliber intraplacental vessels and subplacental vascularity can be seen. On MR imaging, placenta is mostly isointense to the myometrium on T1-weighted images and hyperintense to the myometrium on T2-weighted (T2W) images ( Fig. 5 ). Sometimes, the pregnant uterus can develop vascular congestion, in which case the myometrium demonstrates T2-hyperintense appearance. In such cases, the placenta relatively seems iso- to hypointense to the myometrium (see Fig. 5 ). With increasing gestational age, structure of the cotyledons becomes more apparent and results in decreased signal intensity to intermediate signal intensity compared with the surrounding myometrium ( Fig. 6 ). , First and second trimester placentas are very homogeneous in their appearance but with development of this lobular pattern, the placenta becomes less homogeneous in appearance, as thin hypointense septa become apparent between the lobules on T2W images (see Fig. 6 ). Placental septa and cotyledons are more often visible when MR imaging is performed with a 3 T system.
The placental-myometrial interface is demonstrated as a retroplacental clear space on US and as T2-hypointense interface on MR imaging. Given the isointensity of the placenta to the myometrium on T1-weighted images, the interface is not well seen and is best evaluated on T2W sequences. The normal subplacental vascularity can be seen as multiple flow voids in this subplacental space. A few flow voids can be present within the placenta adjacent to the umbilical cord insertion. The myometrium has a variable thickness and thins as the pregnancy progresses. The underlying myometrial wall thins as the pregnancy advances, and this finding alone does not imply PASD. The myometrium naturally thins at sites of compression, such as adjacent to the maternal spine and aorta, appearing as a single thin layer of uniform signal on T2W images. In addition, the myometrium is expected to thin as the gestation progresses, especially at the site of previous scars.
Imaging protocols
Ultrasound
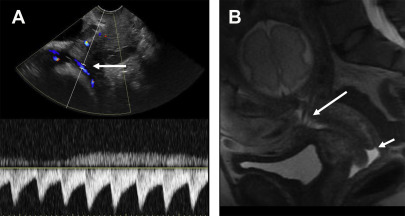
US images should evaluate the entire placenta, and images should be acquired documenting that the entire placenta has been evaluated. Grayscale as well as Doppler imaging should be used. Based on body habitus and depth of the placenta, evaluation with a curvilinear 2 to 6 Megahertz (mHz) and 9 mHz linear transducers can be performed. , In all pregnancies, placenta should be evaluated for the location of implantation, proximity to the cesarean section scar (if applicable), placenta previa or vasa previa, succenturiate lobe, and shape and thickness of the placenta. After this general evaluation, particularly in patients with history of uterine intervention such as cesarean section, myomectomy, embolization, or Asherman syndrome, attention should be drawn to specific findings of PASD such as placental heterogeneity, irregular lacunes or placental lakes, loss of retroplacental clear space/subplacental lucency, myometrial thinning, abnormal subplacental and intraplacental vascularity, placental bulge, and extrauterine invasion (such as that into the bladder or the parametrium). Studies have shown improved patient outcomes when targeted evaluation of the placenta is performed in patients with suspected PASD. Details of these findings are discussed later in this article. In addition, with placental evaluation, it is imperative to evaluate the area of the internal os with color Doppler imaging to evaluate for any aberrant vessels at this location. If any vessels are present, they can be further evaluated with spectral Doppler to look for their maternal versus fetal origin, based on heart rate observations. Vessels demonstrating arterial waveforms at fetal heart rate are highly suspicious for vasa previa.
MR Imaging
The authors’ institutional MR imaging protocol for placental imaging is summarized in Table 1 . In brief, a combination of T2 (not fat suppressed) and T1 images are necessary. Most of the findings for PASD and placental masses are evident on nonfat-suppressed T2W images. T1 images are essential to evaluate for intrinsic hyperintensity secondary to hemorrhage in PASD and to detect the presence of fat in placental masses. Occasionally, fat-suppressed T1 images may be needed, when evaluating for the presence of fat in placental masses. The role of diffusion-weighted imaging in placental imaging is still evolving. In the author’s experience, DWI is particularly helpful in cases with severe myometrial vascular congestion, to help delineate the placental-myometrial interface. In this scenario, the placenta demonstrates hyperintensity, whereas the myometrium does not and hence making their interface better visualized. Technical details of MR imaging for the placenta are summarized in Michael A. Ohliger and Hailey H. Choi’s article, “ Imaging Safety and Technical Considerations in the Reproductive Age Female ,” in this issue.
| Coverage | TR | TE | Flip | NEX | Slice | Matrix | FOV | Phase | Oversample | |
|---|---|---|---|---|---|---|---|---|---|---|
| Patient should drink water before commencing study | ||||||||||
| Coronal, axial, and sagittal single-shot fast spin echo (ssFSE) | Uterus to below cervix | 2000 | 100 | X | X | 4/0 | 384×256 | 36 | R > L | PE FOV 1.0 |
| Axial LAVA FLEX or mDIXON DUAL ECHO | Center over the placenta | 4.2 | 1.2 | 15 | 1 | 3/0 | 260×256 | 34 | A > P | PE FOV 1.1 |
| Coronal ssFSE (nonpropeller) | High-resolution imaging (reduced field of view), center over the placenta | 2000 | 100 | X | X | 4/0 | 384×256 | 26–28 | R > L | PE FOV 1.0 |
| Axial T2 FSE (nonpropeller) | No fat saturation, high-resolution imaging (reduced field of view), center over the placenta | 4000 | 120 | 120 | 2 | 4/0 | 320×256 | 24 | R > L | NPW |
| Sagittal T2 FSE propeller | No fat saturation, high-resolution imaging (reduced field of view), center over the placenta | 11,000 | 74 | 2 | 4/0 | 256×256 | 24 | |||
| Axial and sagittal diffusion-weighted imaging (DWI) | Multiple b-values of 0, 50, 500, 1000: ADC maps Routine field of view | 5000 | 30.5 | 2 | 6/0 | 80×80 | 34 | PE FOV 1 | ||
Imaging findings/pathology
Placenta Accreta Spectrum
PASD is a spectrum of disorders where the placenta adheres to the underlying myometrium and hence does not separate at the time of delivery, leading to massive hemorrhage, which can be life threatening to the mother. The spectrum includes accreta (where the placenta is attached directly to the myometrium, without intervening decidua), increta (with myometrial invasion), and percreta, where the placenta extends outside the uterine serosa and possibly into adjacent organs such as the bladder and the parametrium. International Federation of Gynecology and Obstetrics has proposed a combined clinical-pathologic classification, which includes both intraoperative observations as well as findings on gross pathology. Often relying on pathology alone can lead to erroneous estimation of the severity of the findings, leading to this combined system. No single imaging feature has been shown to be diagnostic for PASD, and usually a combination of multiple findings exists, alerting the reviewers to the correct diagnosis.
Ultrasound
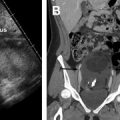
On US some of the commonly reported signs are the presence of multiple placental lakes with irregular margins ( Fig. 7 ), the loss of retroplacental clear space, between the placenta and the myometrium (see Fig. 7 ), and presence of placenta previa (see Fig. 7 ). Other features include heterogeneous placenta, asymmetry of placental thickness, myometrial thinning, bladder wall interruption, myometrial, and bladder wall hypervascularity (see Fig. 7 ).
Prominent placental lacunes
This is the most commonly reported US finding of abnormal placentation, which is present irrespective of the depth of invasion (see Fig. 7 ). , Placental lacunes are vascular anechoic or hypoechoic structures located within the center of the cotyledons. Although a few of these are often present in normal placentae, imaging findings of PASD represent a spectrum of worsening appearance, as they become larger, irregular, and concentrated in the area of invasion and can demonstrate slow internal flow on real-time imaging. , These are also often referred as “placental lakes” and give the placenta the classic “moth-eaten” appearance. ,
Loss of retroplacental clear space
The normal placental-myometrial interface seems hypoechoic on gray-scale US, which represents the normal decidua basalis. With PASD, this clear space is obliterated (see Fig. 7 ), , and approximately 70% of cases will show this finding. In some cases, this area can have prominent subplacental vascularity.
Myometrial thinning
In cases of PAS, myometrium may be thinned to submillimeter levels and actually becomes undetectable in more severe cases (see Fig. 7 ). , It is reported to occur in about 50% of cases, which may be reflective of US changes that happen at the more invasive end of the spectrum. ,
Placental bulge sign
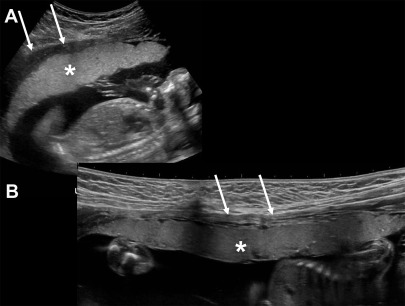
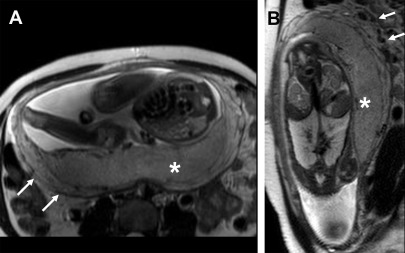
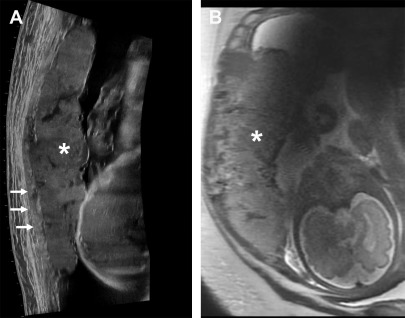
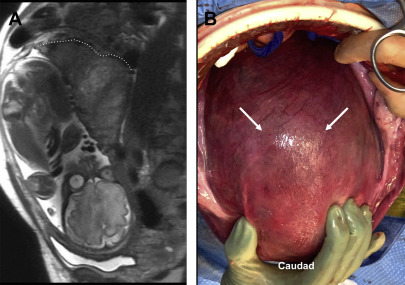
With deeper depths of invasion, the placenta may bulge outward, creating an hourglass or snowman configuration of the uterine contour. Along with myometrial thinning, this finding highly suggests myometrial invasion ( Figs. 8 and 9 ).
Related posts:
 Imaging Safety and Technical Considerations in the Reproductive Age Female
Imaging Safety and Technical Considerations in the Reproductive Age Female
 Magnetic Resonance Imaging of the Female Pelvic Floor
Magnetic Resonance Imaging of the Female Pelvic Floor
 Imaging of Acute Pelvic Pain
Imaging of Acute Pelvic Pain
 Integrated MR Analytical Approach and Reporting of Pelvic Floor Dysfunction
Integrated MR Analytical Approach and Reporting of Pelvic Floor Dysfunction
 Imaging of Postpartum/Peripartum Complications
Imaging of Postpartum/Peripartum Complications
 Nonfetal Imaging During Pregnancy
Nonfetal Imaging During Pregnancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


