Magnetic resonance imaging (MRI) provides excellent delineation of the bones of the elbow and the surrounding soft tissue structures. The components of the elbow can be divided into osseous structures, the joint capsule and ligaments, muscles and tendons, and nerves. In this article, the authors review the normal anatomy and appearance of these structures on MRI as well as the anatomic variants that should be recognized and distinguished from pathologic entities.
Magnetic resonance imaging (MRI) provides excellent delineation of the bones of the elbow and the surrounding soft tissue structures. The components of the elbow can be divided into osseous structures, the joint capsule and ligaments, muscles and tendons, and nerves. In this article, the authors review the normal anatomy and the appearance of these structures on MRI as well as the anatomic variants that should be recognized and distinguished from pathologic entities.
Protocol
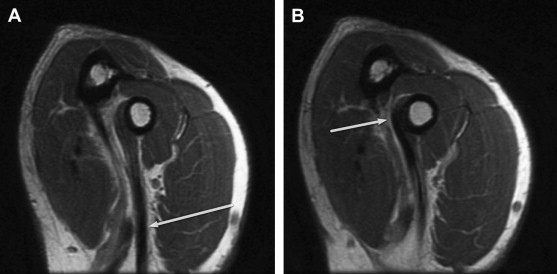
Axial, coronal, and sagittal images are acquired using T1- and T2-weighted images ( Table 1 ). The axial images must include the radial tuberosity where the biceps tendon attaches. Typically, patients are placed in supine position with the arm to their side, and as a result, excellent field homogeneity is required for off-center fat suppression. Although the patient can alternatively be positioned prone with the arm extended overhead, this position is less well tolerated and can also introduce motion degradation artifact. The distal biceps brachii tendon takes an oblique course and is therefore susceptible to partial volume-average effects and difficult to visualize on a single image. The extent of the tendon can be better imaged with the flexed abducted supinated view, whereby the elbow is flexed with the shoulder abducted and the forearm in supination ( Fig. 1 ).
| Pulse Sequence | Field of View (cm) | Slice Thickness (mm) | Matrix | TR/TE |
|---|---|---|---|---|
| Coronal T1 | 14 | 3 | 256 × 192 | 500–700/12–14 |
| Coronal T2 FS | 14 | 3 | 256 × 256 | >4000/54 |
| Axial T1 | 12–14 | 3 | 256 × 256 | 400–750/10–11 |
| Axial T2 FS | 12–14 | 3 | 256 × 256 | >3500/47 |
| Sagittal T2 FS | 14–16 | 3 | 256 × 256 | >3500/47–52 |
Osseous structures
The elbow joint is composed of three bones (humerus, radius, and ulna) that form three articulations (ulnohumeral, radiohumeral, and radioulnar) within a common joint capsule. The ulnohumeral and radiohumeral articulations allow for flexion and extension of the forearm. The radiohumeral and radioulnar articulations permit pronation and supination of the forearm.
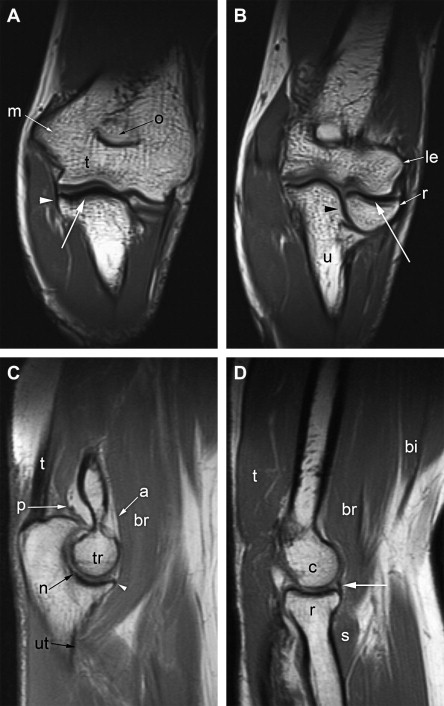
The tubular shaft of the humerus flares distally to form the medial and lateral condyles. As the condyles sweep outward, they form paired bony protuberances, the medial and lateral epicondyles, that serve as attachment sites for ligaments and tendons. The most distal aspects of the condyles are the articular surfaces, the medial trochlea and lateral capitellum. The trochlea is the more central and larger of the two and is shaped like a pulley with central concavity and flared margins. The trochlea articulates within the crescent trochlear notch along the anterior surface of the proximal ulna, forming a hinge joint that permits flexion and extension. The proximal aspect of the trochlear notch is formed by the olecranon, whereas the distal aspect is the coronoid process. Dorsal and ventral indentations above the trochlea, which are the olecranon fossa and coronoid fossa, receive these processes when the elbow is in maximal extension or flexion, respectively. The capitellum is a nearly spherical eminence at the distal aspect of the lateral condyle that articulates with the slightly cup-shaped end of the radial head, permitting both flexion and extension and rotation of the radius with respect to the humerus. The radial head has the form of a disk attached to the tapered neck of the proximal radius. This disk articulates with the radial notch of the proximal ulna on the lateral surface of the coronoid process, allowing for axial rotation of the radius with respect to the ulna. The radial fossa is an indentation above the capitellum that accepts the head of the radius when the elbow is in maximal flexion. The relationships between the various osseous structures of the elbow are well depicted on coronal and sagittal magnetic resonance images ( Fig. 2 ).
Osseous structures
The elbow joint is composed of three bones (humerus, radius, and ulna) that form three articulations (ulnohumeral, radiohumeral, and radioulnar) within a common joint capsule. The ulnohumeral and radiohumeral articulations allow for flexion and extension of the forearm. The radiohumeral and radioulnar articulations permit pronation and supination of the forearm.
The tubular shaft of the humerus flares distally to form the medial and lateral condyles. As the condyles sweep outward, they form paired bony protuberances, the medial and lateral epicondyles, that serve as attachment sites for ligaments and tendons. The most distal aspects of the condyles are the articular surfaces, the medial trochlea and lateral capitellum. The trochlea is the more central and larger of the two and is shaped like a pulley with central concavity and flared margins. The trochlea articulates within the crescent trochlear notch along the anterior surface of the proximal ulna, forming a hinge joint that permits flexion and extension. The proximal aspect of the trochlear notch is formed by the olecranon, whereas the distal aspect is the coronoid process. Dorsal and ventral indentations above the trochlea, which are the olecranon fossa and coronoid fossa, receive these processes when the elbow is in maximal extension or flexion, respectively. The capitellum is a nearly spherical eminence at the distal aspect of the lateral condyle that articulates with the slightly cup-shaped end of the radial head, permitting both flexion and extension and rotation of the radius with respect to the humerus. The radial head has the form of a disk attached to the tapered neck of the proximal radius. This disk articulates with the radial notch of the proximal ulna on the lateral surface of the coronoid process, allowing for axial rotation of the radius with respect to the ulna. The radial fossa is an indentation above the capitellum that accepts the head of the radius when the elbow is in maximal flexion. The relationships between the various osseous structures of the elbow are well depicted on coronal and sagittal magnetic resonance images ( Fig. 2 ).
Joint capsule and ligaments
A common joint capsule surrounds all three joints of the elbow. The capsule is composed of a more superficial fibrous layer and a deeper synovial layer. There are three fat pads between these two layers ( Fig. 3 ). The two anterior fat pads are situated within the coronoid fossa and radial fossa, whereas the posterior fat pad sits within the olecranon fossa. The ligaments of the elbow range from focal areas of thickening of the capsule to more discrete fibers visible on MRI. As the primary motion of the elbow is flexion and extension, the anterior and posterior aspects of the joint capsule are thin. The major stabilizers of the elbow are the medial (ulnar) and lateral (radial) collateral ligament complexes.
The ulnar collateral ligament, also known as the medial collateral ligament, consists of three ligamentous bundles, the anterior, posterior, and transverse bundles. The anterior bundle is the major medial stabilizer of the elbow and is the only component of the ulnar collateral ligament seen as a discrete ligament on MRI. As best demonstrated on coronal images ( Fig. 4 ), the anterior bundle arises from the inferior margin of the medial epicondyle and attaches to the medial aspect of the coronoid process at the sublime tubercle. The posterior bundle is a thickening of the joint capsule that extends from below the medial epicondyle to the medial olecranon. The transverse bundle consists of fibers extending from the inferior aspects of the anterior and posterior bundles, that is, from the olecranon to the coronoid process, and does not contribute to elbow stability.