Normal Physiologic FDG Uptake Patterns
Todd M. Blodgett, MD
Alex Ryan, MD
Barry McCook, MD
Key Facts
Terminology
FDG activity associated with normal anatomical structures or benign processes
Imaging Findings
FDG uptake in primary neoplasms is usually greater than that observed in even the most metabolically active normal structures
However, overlap does occur and may confound interpretation
Symmetry is not always a reliable indicator of physiologic processes
Physiologic uptake will often be asymmetrical
Post-surgical patients often demonstrate anatomic asymmetry
Any physiologic FDG activity should correspond to otherwise normal-appearing structures
Correlation with CT is absolutely essential to minimize misinterpretation
Top Differential Diagnoses
Head and Neck Structures with Variable FDG Uptake
Pterygoid Muscles
Lymphoid Tissue in Waldeyer Ring
Thymus
Fat
Post-Operative Altered Physiologic States
Lymphoid Tissue
Clinical Issues
Brown fat more common in women during the winter months
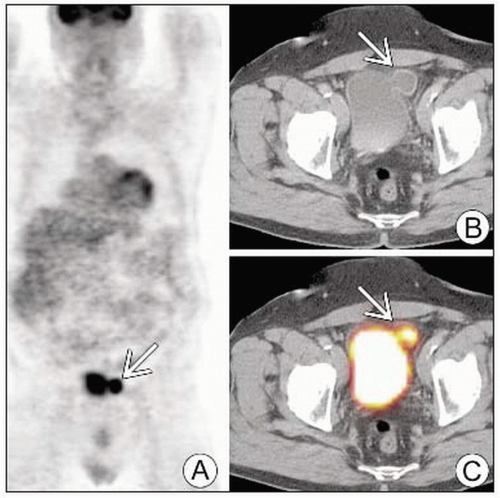 Multiple images (A, B, C) show the typical appearance of a bladder diverticulum  . . |
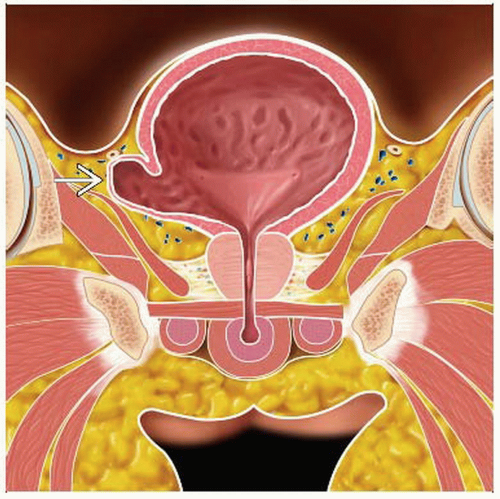 Graphic shows a representation of a right-sided bladder diverticulum  , similar in structure to the one depicted in the previous images. , similar in structure to the one depicted in the previous images. |
TERMINOLOGY
Definitions
FDG activity associated with normal anatomical structures or benign processes
IMAGING FINDINGS
General Features
Best diagnostic clue
FDG uptake in primary neoplasms is usually greater than that observed in even the most metabolically active normal structures
However, overlap does occur & may confound interpretation
Morphology: Any physiologic FDG activity should correlate with otherwise normal-appearing structures
Imaging Recommendations
Best imaging tool: Correlation with CT is absolutely essential to minimize misinterpretation
Protocol advice
Sedation and neck immobilization may help reduce physiologic FDG activity in the skeletal muscles
Sedation is inconvenient for patients and may not completely eliminate physiologic uptake
Patients generally instructed to remain quiet during FDG uptake phase to limit vocal cord uptake
Nuclear Medicine Findings
Symmetry
Interpreting physician often relies on symmetry or location to differentiate between physiologic and pathologic FDG accumulations
Symmetry is not always a reliable indicator of physiologic processes
Physiologic uptake will often be asymmetrical
Several malignancies can present with strikingly symmetrical FDG uptake
Post-surgical patients often demonstrate anatomic asymmetry
DIFFERENTIAL DIAGNOSIS
Head and Neck Structures with Variable FDG Uptake
Nasal turbinates
Pterygoid muscles
Extraocular muscles
Parotid and submandibular glands
Lymphoid tissue in Waldeyer throat ring
Chest Structures with Variable Uptake
Thymus
Heart
Thorax muscles
Many are age- or activity-dependent
Thyroid Gland
Normal thyroid has variable appearance using FDG PET
May demonstrate diffuse, focal, asymmetric, or virtually no uptake
Each of the above patterns may be seen in physiologic, benign, and pathologic processes
Focal uptake
Relatively nonspecific
Malignancy, including second primary
Adenomatous processes
Toxic thyroid adenoma
Recommended that all patients with nodules ≥ 10 mm and all those with intense asymmetric FDG uptake be referred for biopsy
Diffuse symmetric uptake
Seen in normal thyroid
Occasionally seen with diffuse goiter
Chronic autoimmune thyroiditis
Salivary Glands
FDG is taken up by salivary glands and excreted into saliva
Parotid and submandibular glands normally demonstrate symmetric mild-moderate uptake
Normal glands may also show no uptake
Asymmetric uptake seen in
Patients who have undergone surgical removal of a gland
Patients with primary or metastatic lesions to the glands
FDG-avid parotid tumors include
Warthin tumor
Pleomorphic adenoma
Primary parotid lymphoma
Nonmalignant uptake
Infectious etiologies
Granulomatous disorders (e.g., sarcoidosis)
Benign and malignant parotid tumors cannot be distinguished with PET/CT alone because of high false positive rates
In addition, several salivary gland malignancies have little or no FDG avidity
Lack of FDG uptake does not exclude malignancy
Malignancy can sometimes cause bilateral FDG uptake in the parotid or submandibular glands or in intraparotid lymph nodes
Mimics a physiologic pattern of uptake
Muscles of Neck and Face
Neck muscle uptake a common diagnostic dilemma
Muscular uptake can frequently be distinguished from malignant nodal uptake by identifying characteristic pattern of linear symmetric uptake
However, muscles often have more focal uptake patterns
Fusion images often localize FDG uptake to the myotendinous junction
Can be difficult to distinguish from abnormal lymph nodes
Intense asymmetric uptake may be seen in sternocleidomastoid muscle, mimicking enlarged node
Inspection of coronal or sagittal reconstructions may reveal linearity
Inferior obliquus capitis muscle frequently demonstrates asymmetric tracer uptake
Uptake may appear focal on coronal images
Linear nature evident in axial plane
Extreme posterior position of these muscles often helpful in identifying them as the source of FDG uptake
Muscles of facial expression may also demonstrate linear FDG activity
Close inspection of 3 orthogonal planes is essential to avoid misdiagnosis
Muscles of Oropharynx and Nasopharynx
Symmetric physiologic uptake seen in pterygoid muscles and muscles of oral floor
May mimic malignancy when asymmetric
Lingual uptake is common and may appear as diffuse or bilateral symmetrical focal uptake
Often inseparable from slightly more superior palatal mucosal uptake
Can be differentiated on PET/CT images
Laryngeal Muscles
Talking during FDG uptake period causes tracer accumulation in vocal cords and muscles of phonation
Cricopharyngeus muscle can also appear as focal area of uptake
Coughing during uptake period produces activity in pharyngeal constrictor muscles and vocal cords
In patients with head and neck malignancies, thyroid cancer, or lymphoma, it can be very difficult to distinguish physiologic from pathologic uptake
Fat
Brown fat is metabolically active and may demonstrate FDG uptake
Theorized to be useful for heat generation
Generally easily localized by PET/CT
Brown fat can be distinguished from other tissue if Hounsfield units measure fat attenuation, -50 to -150 HU
Warming patients may reduce uptake in this tissue
More common in women and observed more commonly in winter months
Commonly seen in the following areas
Neck
Retrocrural
Perirenal
Left paratracheal
Post-Operative Altered Physiologic States
Knowledge of prior surgeries and surgical complications is essential for properly interpreting foci of FDG in the head and neck
e.g., recurrent laryngeal nerve damage and intense FDG uptake by compensatory effort of contralateral vocal cord
Lymphoid Tissue
Lymphatic structures in head and neck
Waldeyer throat ring (adenoids, palatine tonsils, and lingual tonsils)
Lymph nodes
Lymphatic channels
Physiologic uptake can be seen in any lymphatic structures in head and neck
Related to uptake in macrophages and lymphocytes
Malignancy and hyperplasia may have similar symmetric appearance
Malignancy usually presents with asymmetric FDG uptake
May appear with or without significant anatomic abnormalities
Uptake in Waldeyer ring will often be asymmetric
When accidentally infiltrated into subcutaneous tissue, FDG can be transported through lymphatic channels and produce lymphangiogram effect
May accumulate in lymph nodes of axilla and supraclavicular area
Mucosa
Mucosa of oropharynx and nasopharynx often demonstrates physiologic FDG uptake
Rarely causes diagnostic problems because almost invariably superficial along mucosal plane in linear configuration
Esophagus
Generally not very FDG avid
Several benign infectious/inflammatory processes can cause spectrum of FDG uptake
Distal esophagitis: Mild focal uptake
Radiation injury (and other etiologies that affect entire esophagus): Diffuse linear intense FDG uptake
Great majority of esophageal malignancies are visualized as focal to short segment areas of intense FDG uptake
Exception: Some gastroesophageal junction adenocarcinomas that arise in cardia of stomach
Lung
On attenuation-corrected (AC) images, lungs appear very light with little FDG uptake
Benign lung lesions may mimic a malignant pulmonary nodule
Tuberculosis
Pneumonia (viral, bacterial, fungal)
Collagen vascular diseases
Vasculitides
Sarcoidosis
Silicosis
Most malignant lesions > 1 cm tend to have higher SUVs (> 2.5) than benign lesions
However, there are reports of benign lesions with SUVs well above 5
Some malignancies are poorly FDG avid, including bronchoalveolar cell carcinoma
PET/CT imaging allows anatomic correlation that can help secure diagnosis
Thymus
Often visible in pediatric population as V-shaped structure just above heart on coronal image, with mild to intense FDG uptake
In adult patients, thymus typically not visible on FDG PET or CT
Causes of thymic uptake in adult
Thymic carcinoma
Thymic rebound after illness or chemotherapy
Thymic hyperplasia
Heart
Most important factor determining heart uptake is whether patient has fasted
Most protocols instruct patient to fast for 4-6 hours prior to scan
Fasting reduces cardiac glucose dependence
In non-fasting patient, left ventricular FDG uptake can obscure a lesion directly adjacent to left ventricle
Left ventricle is the only chamber with appreciable activity on PET scan
Abdominal Muscle
Muscle generally exhibits more FDG uptake when exercised during or preceding FDG injection
Muscles that may appear asymmetrical include crus of diaphragm and strap muscles
Stomach
Variable physiologic FDG activity ranging from minimal to fairly intense
Uptake typically distributed throughout gastric mucosa
Inflammatory processes such as gastritis can increase uptake
Liver/Spleen
Both organs have similar physiologic FDG activity, usually mild and diffuse
Focal areas worrisome for neoplastic uptake
Causes of diffuse splenic uptake
Erythropoietin
Chemotherapy
G-CSF
Bowel
One of the most difficult structures in which to differentiate physiologic from pathologic uptake
Typical appearance is linear in 3 orthogonal planes, ranging from mild to intense
Focal bowel activity
Can be physiologic
Should raise suspicion of neoplastic process (particularly if the rest of the bowel has no activity)
Most patients should have correlation with colonoscopy or sigmoidoscopy
Polyps may have focal uptake irrespective of degree of malignancy
Focal lesions adjacent to normal linear bowel uptake often cannot be separated as distinct structures
Uterus
Patient history is crucial to interpretation
Intense endometrial activity is seen during menstruation
With correct menstrual history, no follow-up is warranted
In postmenopausal patient, intense uptake very concerning for endometrial carcinoma
Fibroids can have focal FDG uptake ranging from minimal to very intense in the setting of degeneration
Ovary
Most patients do not have visible FDG uptake within ovaries
Cases of physiologic uptake have been reported
Benign structures such as corpus luteum cyst can have intense FDG uptake
Correlation with CT is important
Typical appearance of corpus luteum cyst: Thick rind of enhancement in otherwise normal-appearing ovary
Urinary Collecting System
Unlike glucose, FDG is normally excreted in the urinary collecting system
Background uptake in kidneys makes it difficult to distinguish renal masses (such as renal cell carcinoma) from background excretory FDG
Focal ureteral stasis may appear as focal area of FDG uptake and mimic appearance of lymph node
Helpful to have patient void and then repeat 1-2 bed positions through area of uptake
CLINICAL ISSUES
Demographics
Gender: Brown fat more common in women during the winter months
SELECTED REFERENCES
1. Chang JM et al: False positive and false negative FDG-PET scans in various thoracic diseases. Korean J Radiol. 7(1):57-69, 2006
2. Rosenbaum SJ et al: False-positive FDG PET uptake–the role of PET/CT. Eur Radiol. 16(5):1054-65, 2006
3. Truong MT et al: Pitfalls in integrated CT-PET of the thorax: implications in oncologic imaging. J Thorac Imaging. 21(2):111-22, 2006
4. Blodgett TM et al: Combined PET-CT in the head and neck: part 1. Physiologic, altered physiologic, and artifactual FDG uptake. Radiographics. 25(4):897-912, 2005
5. Fukui MB et al: Combined PET-CT in the head and neck: part 2. Diagnostic uses and pitfalls of oncologic imaging. Radiographics. 25(4):913-30, 2005
6. Heiba SI et al: The distinctive role of positron emission tomography/computed tomography in breast carcinoma with brown adipose tissue 2-fluoro-2-deoxy-d-glucose uptake. Breast J. 11(6):457-61, 2005
7. Nakamoto Y et al: Normal FDG distribution patterns in the head and neck: PET/CT evaluation. Radiology. 234(3):879-85, 2005
8. Subhas N et al: Imaging of pelvic malignancies with in-line FDG PET-CT: case examples and common pitfalls of FDG PET. Radiographics. 25(4):1031-43, 2005
Image Gallery
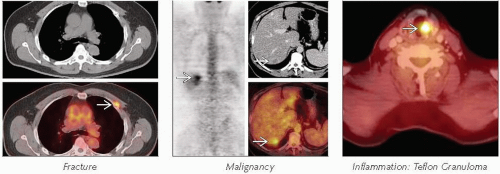 DDx: Focal FDG Activity |
 (Left) Axial CECT shows no abnormalities. (Right) Axial fused PET/CT shows symmetrical intense FDG activity within the lingula tonsils  , compatible with normal physiologic activity. , compatible with normal physiologic activity. |
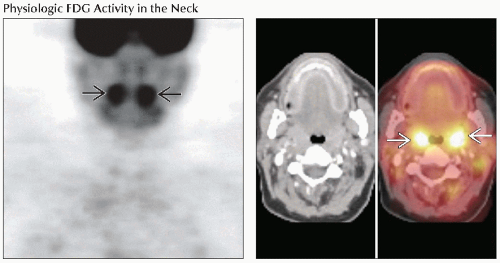 (Left) Coronal PET shows symmetrical intense FDG activity within the palatine tonsils  , compatible with physiologic activity. (Right) Axial images show normal anatomy on the axial CT (left) with corresponding focal intense FDG activity on fused PET/CT (right) in the palatine tonsils , compatible with physiologic activity. (Right) Axial images show normal anatomy on the axial CT (left) with corresponding focal intense FDG activity on fused PET/CT (right) in the palatine tonsils  , compatible with normal physiologic activity. , compatible with normal physiologic activity. |
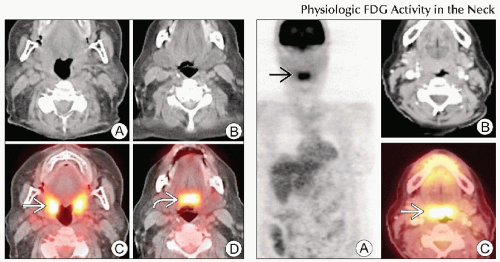 (Left) Axial CT (A, B) and fused PET/CT (C, D) show physiologic activity within the lingual tonsils bilaterally  as well as the palatine tonsils as well as the palatine tonsils  , compatible with normal physiologic activity. (Right) Coronal PET (A) shows intense FDG activity along the midline , compatible with normal physiologic activity. (Right) Coronal PET (A) shows intense FDG activity along the midline  , corresponding to the lingual tonsils , corresponding to the lingual tonsils  on the fused PET/CT image (C). Note that no abnormalities are seen on the CECT (B). on the fused PET/CT image (C). Note that no abnormalities are seen on the CECT (B). |
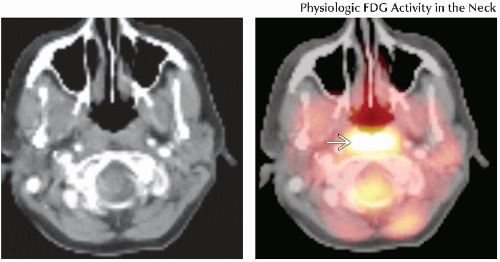 (Left) Axial CECT shows no obvious abnormalities. (Right) Axial fused PET/CT shows diffuse FDG activity within the adenoids bilaterally  , compatible with normal physiologic activity. , compatible with normal physiologic activity. |
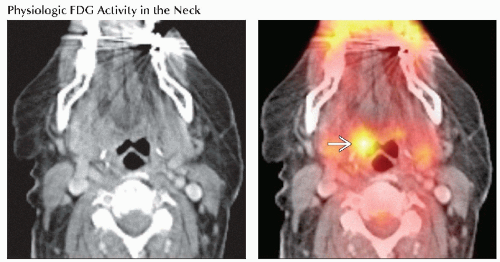 (Left) Axial CECT shows no obvious abnormalities. (Right) Axial fused PET/CT shows focal asymmetrical FDG activity in the right lingual tonsil  . A subsequent biopsy demonstrated hyperplasia. . A subsequent biopsy demonstrated hyperplasia. |
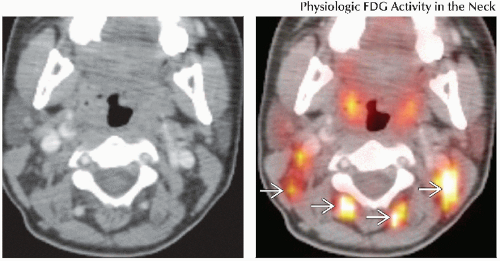
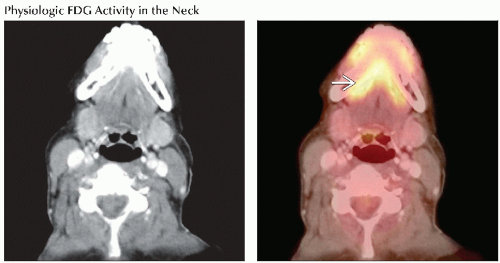 (Left) Axial CECT shows no obvious abnormalities. (Right) Axial fused PET/CT shows bilateral areas of linear intense FDG activity that correspond to the sublingual glands  and are compatible with physiologic activity. and are compatible with physiologic activity. |
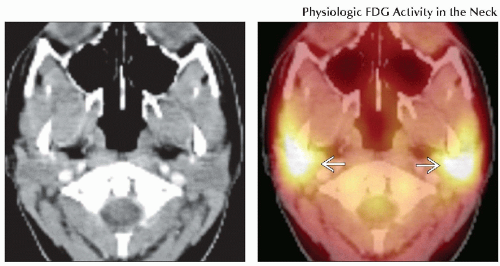 (Left) Axial CECT shows no obvious abnormalities. (Right) Axial fused PET/CT shows intense diffuse symmetrical activity within both parotid glands  , compatible with physiologic activity. , compatible with physiologic activity. |
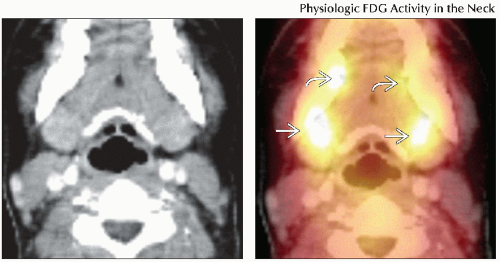 (Left) Axial CECT shows no obvious abnormalities. (Right) Axial fused PET/CT shows intense symmetrical activity within the submandibular glands  , as well as within the sublingual glands , as well as within the sublingual glands  , compatible with physiologic activity. , compatible with physiologic activity. |
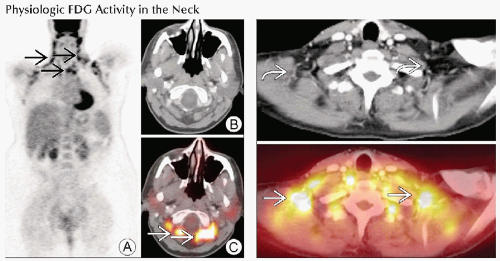
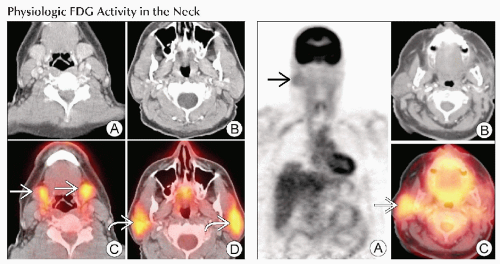 (Left) Axial CT (A, B) and fused PET/CT (C, D) demonstrate intense FDG activity within the submandibular glands  , as well as the parotid glands bilaterally , as well as the parotid glands bilaterally  , compatible with normal physiologic activity. (Right) Coronal PET (A) shows asymmetrical mild to moderately increased FDG activity within the right neck , compatible with normal physiologic activity. (Right) Coronal PET (A) shows asymmetrical mild to moderately increased FDG activity within the right neck  , corresponding to asymmetrical physiologic activity within the right parotid gland , corresponding to asymmetrical physiologic activity within the right parotid gland  on PET/CT (C) in this patient who had a history of a left-sided parotidectomy. Axial CT (B) is normal. on PET/CT (C) in this patient who had a history of a left-sided parotidectomy. Axial CT (B) is normal. |
 (Left) Coronal PET (A) shows diffuse intense FDG activity throughout the thyroid gland  , corresponding to an otherwise normal-appearing thyroid , corresponding to an otherwise normal-appearing thyroid  on axial CT (B) and fused PET/CT (C). Subsequent correlation with thyroid function test showed no abnormalities, suggesting physiologic activity. (Right) Axial fused PET/CT (bottom) shows diffusely increased FDG activity on axial CT (B) and fused PET/CT (C). Subsequent correlation with thyroid function test showed no abnormalities, suggesting physiologic activity. (Right) Axial fused PET/CT (bottom) shows diffusely increased FDG activity  that corresponds to an enlarged left lobe of the thyroid that corresponds to an enlarged left lobe of the thyroid  on axial CT (top), findings compatible with a multinodular goiter. on axial CT (top), findings compatible with a multinodular goiter. |
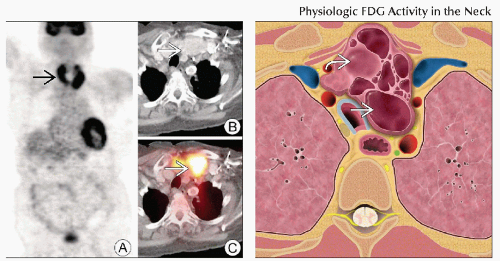 (Left) Coronal PET (A) shows diffusely increased FDG activity throughout both lobes of the thyroid gland  , corresponding to an unenlarged gland with multiple nodules , corresponding to an unenlarged gland with multiple nodules  on axial CT (B) and fused PET/CT (C), compatible with multinodular goiter. (Right) Graphic shows a multinodular goiter with multiple colloid cysts on axial CT (B) and fused PET/CT (C), compatible with multinodular goiter. (Right) Graphic shows a multinodular goiter with multiple colloid cysts  , as well as slightly more nodular soft tissue areas , as well as slightly more nodular soft tissue areas  . . |
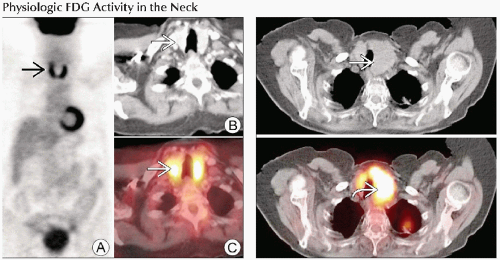
 (Left) Axial CECT shows no obvious abnormalities. (Right) Axial fused PET/CT shows multiple foci of increased FDG activity that correspond to areas of fat attenuation  , compatible with physiologic brown fat. , compatible with physiologic brown fat. |
 (Left) Coronal PET (A) shows extensive foci of increased FDG activity in the neck and supraclavicular/axillary areas
 , corresponding to areas of fat attenuation , corresponding to areas of fat attenuation  on CT (B) and fused PET/CT (C), compatible with brown fat. (Right) Axial fused PET/CT (bottom) shows multiple foci of intense FDG activity in the supraclavicular area on CT (B) and fused PET/CT (C), compatible with brown fat. (Right) Axial fused PET/CT (bottom) shows multiple foci of intense FDG activity in the supraclavicular area  , corresponding to areas of fat attenuation , corresponding to areas of fat attenuation  on the axial CT (top), compatible with physiologic brown fat. on the axial CT (top), compatible with physiologic brown fat.Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|