Nose and Paranasal Sinuses
Daniel Thomas Ginat
Daniel Chow
QUESTIONS

View Answer
1 Answer B.
|

Discussion:
A: The lamina papyracea is the medial orbital wall.
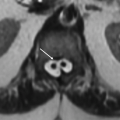
B: The uncinate process is a bony projection alongside the infundibulum.
C: The cribriform plate is the roof of the nasal cavity, through which the olfactory nerves are transmitted. The cribriform plate is composed of a medial and lateral lamella on each side.
D: The inferior turbinate is the largest of the nasal turbinates and is covered by scroll-shaped mucosa that can vary in thickness.
Reference: Vaid S, Vaid N. Normal anatomy and anatomic variants of the paranasal sinuses on computed tomography. Neuroimaging Clin N Am 2015;25(4):527-548.
2 Where does the nasolacrimal duct drain?
A. Frontoethmoid recess
B. Sphenoethmoid recess
C. Middle meatus
D. Inferior meatus
View Answer
2 Answer D. Inferior meatus.
Discussion: The nasolacrimal duct extends from the lacrimal sac to the inferolateral nasal cavity. In particular, tears drain into the inferior meatus, which is located lateral to the inferior turbinate. The frontal, anterior ethmoid, and maxillary sinuses drain into the middle meatus. The frontal sinuses drain into the frontoethmoid recess, while the sphenoid sinuses drain into the sphenoethmoid recess. The sphenoid and posterior ethmoid sinuses then collectively drain into the superior meatus.
Reference: Vaid S, Vaid N. Normal anatomy and anatomic variants of the paranasal sinuses on computed tomography. Neuroimaging Clin N Am 2015;25(4):527-548.
3 Which of the following variants is correctly paired with the potential complication from endoscopic sinus surgery?
A. Lamina papyracea dehiscence: olfactory bulb injury
B. Sphenoid sinus dehiscence: internal carotid artery injury
C. Cribriform plate asymmetry: optic nerve injury
D. Retained Haller cell: persistently obstructed frontal sinus drainage
View Answer
3 Answer B. Sphenoid sinus dehiscence: internal carotid artery injury.
Discussion: There are several important anatomical variants and acquired abnormalities that can compromise the success of endoscopic sinus surgery. Dehiscence of the lamina papyracea can be congenital or acquired through trauma and can predispose to intraorbital injury during surgery, particularly the medial rectus muscle. Depending on the location of a sphenoid sinus dehiscence, the internal carotid artery, optic nerve, and trigeminal nerve are potentially at risk of injury during surgery. An asymmetric, particularly a low-lying, cribriform plate can lead to an increased risk of injury of the olfactory apparatus or adjacent brain parenchyma or branches of the anterior cerebral artery. Haller cells are anterior ethmoid air cells that extend along the floor of the orbits, lateral to the sagittal plane of the lamina papyracea, and can contribute to obstruction of the infundibulum.
Reference: Hoang JK, Eastwood JD, Tebbit CL, et al. Multiplanar sinus CT: a systematic approach to imaging before functional endoscopic sinus surgery. AJR Am J Roentgenol 2010;194(6):W527-W536.

A. Acute invasive fungal rhinosinusitis
B. Allergic fungal sinusitis
C. Pott puffy tumor
D. Mycetoma
View Answer
4 Answer A. Acute invasive fungal rhinosinusitis.
|

Imaging Findings: The axial CT image shows hyperattenuating material within the left maxillary sinus, as well as periantral fat infiltration (arrows).
Discussion: Acute invasive fungal rhinosinusitis is an aggressive infection often caused by Aspergillus species and Mucor species in diabetic and/or immunocompromised individuals. The presence of periantral fat infiltration, bone dehiscence, orbital invasion, septal ulceration, pterygopalatine fossa, nasolacrimal duct, and lacrimal sac involvement are potential signs of acute invasive fungal rhinosinusitis on imaging. On the other hand, allergic fungal sinusitis is a relatively common and indolent type I IgE-mediated allergic response to inhaled fungal spores and manifests as hyperattenuating allergic mucin with the sinuses.
Pott puffy tumor represents a subperiosteal abscess and/or epidural abscess associated with frontal osteomyelitis and sinusitis.
A mycetoma is a fungus ball, which characteristically contains calcifications that can be visible on CT.
Reference: Middlebrooks EH, Frost CJ, De Jesus RO, et al. Acute invasive fungal rhinosinusitis: a comprehensive update of CT findings and design of an effective diagnostic imaging model. AJNR Am J Neuroradiol 2015;36(8):1529-1535.

A. Osteoma
B. Mucocele
C. Paget disease
D. Fibrous dysplasia
View Answer
5 Answer A. Osteoma.
|

Imaging Findings: The axial CT image shows a mass with very high attenuation bone and areas of lower attenuation in the expanded frontal sinuses.
Discussion: Osteomas are benign tumors that characteristically display very dense bone formation, but may also contain lower attenuation fibrous areas. These lesions most commonly occur in the frontal and ethmoid sinuses. Giant osteomas can expand the sinuses and can be complicated by pneumocephalus and meningitis.
Mucoceles can also expand the paranasal sinuses, but do not display bone attenuation.
Paget disease can contain areas of dense bone, producing a “cotton wool” appearance, but arises from the skull itself rather than from within the sinus and tends to be a more diffuse process.
Fibrous dysplasia can be expansile and contain ground-glass components, but does not contain such dense bone as in osteomas.
Reference: Earwaker J. Paranasal sinus osteomas: a review of 46 cases. Skeletal Radiol 1993;22(6):417-423.

A. Rhabdomyosarcoma
B. Encephalocele
C. Juvenile nasal angiofibroma
D. Chondrosarcoma
7 Which of the following is true regarding juvenile nasal angiofibroma?
A. It is a malignant neoplasm.
B. It is avascular.
C. It arises from foramen rotundum.
D. It can erode bone.
View Answer
7 Answer D. It can erode bone.
|

Discussion: Please refer to answer 6.
Imaging Findings: Axial fat-suppressed T2-weighted and postcontrast T1-weighted MR images shows an avidly enhancing mass with prominent flow voids in the left nasal cavity and nasopharynx, centered at the sphenopalatine foramen (arrows).
Discussion: Juvenile nasal angiofibromas are benign, vascular tumors that classically occur in young males presenting with epistaxis. The tumors arise from the sphenopalatine foramen and extend into the posterior nasal cavity and pterygopalatine fossa. Furthermore, juvenile nasal angiofibromas often erode bone of the medial pterygoid plate, which can be depicted on CT. On MRI, flow voids and intense contrast enhancement are typical. The lesions can be amenable to embolization prior to surgery.
Rhabdomyosarcomas are among the most common pediatric head and neck malignancies and can appear as destructive soft tissue tumors.
Encephaloceles are herniations of brain tissue along with variable amounts of cerebrospinal fluid. MRI is useful for depicting the intracranial connections.
Chondrosarcomas are unusual in the sinonasal region and appear as soft tissue tumors with calcified matrix and may erode or remodel the sinus walls.
Reference: Lloyd G, Howard D, Lund VJ, et al. Imaging for juvenile angiofibroma. J Laryngol Otol 2000;114(9):727-730.
8 Which is the most likely diagnosis based on the image below?
 Image courtesy of Dr. Jason Johnson. |
A. Nasopharyngeal carcinoma
B. Nasal polyposis
C. Esthesioneuroblastoma
D. Inverted papilloma
View Answer




8 Answer C. Esthesioneuroblastoma.
|

Imaging Findings: Coronal T2-weighted MRI shows a bulky sinonasal tumor with intracranial extension and associated cysts along the intracranial margin (arrows).
Discussion: Esthesioneuroblastoma (ENB), is a malignant tumor of neural crest origin, and arises from the olfactory epithelium of the superior nasal cavity. It has a bimodal age of presentation in the second and sixth decades. On CT, it presents as soft tissue mass in the nasal vault, often with bony destruction. MRI is superior to define the extent of tumor intracranially and to differentiate tumor from entrapped secretions. The presence of cysts along the intracranial margin of a sinonasal mass is highly suggestive of esthesioneuroblastoma.
Nasal polyposis is associated with allergic rhinitis and can appear as multiple mass lesions with peripheral enhancement due to inflamed mucosa.
Nasopharyngeal carcinoma is often associated with EBV infection, more commonly occurs in adults, and typically arises from the fossa of Rosenmuller.
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
