Presentation and Presenting Images
A 52-year-old female presents for screening mammography. She has a history of bilateral breast cancer with her most recent cancer, involving her right breast, treated 5 years ago.
30.2 Key Images
( ▶ Fig. 30.3, ▶ Fig. 30.4, ▶ Fig. 30.5, ▶ Fig. 30.6)
30.2.1 Breast Tissue Density
There are scattered areas of fibroglandular density.
30.2.2 Imaging Findings
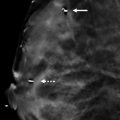
In the lower outer quadrant of the right breast, there is an oval mass at the edge of the film that has a wire marking the skin incision overlying it. This reflects her prior postsurgical changes and the partial breast irradiation (brachytherapy). On first examination of the digital mammograms of the right breast, there appears to be nothing new. Looking at the tomosynthesis images, an irregular mass with obscured and indistinct margins can be identified at the 12 o’clock location in the posterior depth ( ▶ Fig. 30.5 and ▶ Fig. 30.6). In retrospect, these areas can be identified on the conventional digital mammograms ( ▶ Fig. 30.3 and ▶ Fig. 30.4).
30.3 BI-RADS Classification and Action
Category 0: Mammography: Incomplete. Need additional imaging evaluation and/or prior mammograms for comparison.
30.4 Diagnostic Images
( ▶ Fig. 30.7, ▶ Fig. 30.8, ▶ Fig. 30.9, ▶ Fig. 30.10, ▶ Fig. 30.11, ▶ Fig. 30.12, ▶ Fig. 30.13)
30.5 Imaging Findings
The indistinct mass is best demonstrated on the diagnostic mediolateral oblique (MLO) spot-compression and left mediolateral (LML) mammograms ( ▶ Fig. 30.8 and ▶ Fig. 30.9). The surrounding tissues do not interfere as much as they do on the craniocaudal (CC) view ( ▶ Fig. 30.7), obscuring the mass. There appears to be architectural distortion associated with the 1.1 × 1.5 × 1.2 cm irregular mass with indistinct margins located at 12 o’clock. Targeted ultrasound reveals a 1.2 × 1.3 × 0.9 cm irregular hypoechoic mass with angular margins at the 12 o’clock location, 6 cm from the nipple ( ▶ Fig. 30.10 and ▶ Fig. 30.11). This mass was biopsied. The ribbon clip is located at the site of the mass ( ▶ Fig. 30.12 and ▶ Fig. 30.13), which was seen best on the tomosynthesis images ( ▶ Fig. 30.5 and ▶ Fig. 30.6).
30.6 BI-RADS Classification and Action
Category 4C: High suspicion for malignancy
30.7 Differential Diagnosis
Invasive ductal carcinoma (IDC): The imaging characteristics support a diagnosis of cancer. On biopsy, this mass was a grade 2 IDC.
Postoperative scar: This patient has a history of bilateral treated breast cancers. Her right breast cancer site was marked with a skin marker, which locates it in a different quadrant (lower outer) of the breast than the findings. Thus, this is not a likely diagnosis.
Metastasis: Metastasis to the breast is rare (0.5 – 6.6% of all breast malignancies). Occasionally it is the presenting lesion of an unknown primary cancer with the most common being lymphoma or melanoma. This patient does not have any other cancers. If a biopsy yielded this pathology, further systemic evaluation of the patient would be required.
30.8 Management and Digital Breast Tomosynthesis Principles
In this case, digital breast tomosynthesis (DBT) performed better at identifying and localizing the right breast mass.
Some cancers can be effaced on conventional spot-compression images. It is important that if the DBT imaging is concerning, even with a negative diagnostic conventional mammogram, that an ultrasound be performed. This can aid in diagnosing mammographically occult cancers.
DBT is helpful with triangulation of lesions, especially within dense breast tissue which may obscure the lesion in one or both projections.
It is important to remember that not all cancers will be detected on DBT. Evaluation should be directed to the most suspicious imaging findings whether on DBT or full-field digital mammography (FFDM).
30.9 Further Reading
[1] Dershaw DD. Breast imaging and the conservative treatment of breast cancer. Radiol Clin North Am. 2002; 40(3): 501‐516 PubMed
[2] Weinstein SP, Orel SG, Pinnamaneni N, et al. Mammographic appearance of recurrent breast cancer after breast conservation therapy. Acad Radiol. 2008; 15(2): 240‐244 PubMed

Fig. 30.1 Right craniocaudal (RCC) mammogram.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


