Orbit
Addressing normal anatomy, the optic foramen (the opening of the optic canal) lies at the orbital apex and contains the optic nerve and the ophthalmic artery. The superior orbital fissure lies inferolateral to the optic canal and contains the oculomotor (CN III), trochlear (CN IV), and abducens (CN VI) nerves, together with the ophthalmic nerve (CN V1) (and branches therein) and the ophthalmic veins. The inferior orbital fissure lies more inferiorly, and slightly laterally, and contains the maxillary nerve (CN V2). The medial wall of the orbit is referred to as the lamina papyracea (paper thin). The extraocular muscles include the superior, inferior, medial, and lateral recti, together with the superior and inferior obliques and the levator palpebrae superioris. The superior oblique muscle is the longest and thinnest, passing anteriorly and medially through the trochlea and then turning posterolaterally and downward to insert on the lateral sclera. The inferior oblique, the only muscle not to originate from the orbital apex, originates from the maxilla. The levator palpebrae superioris muscle lies between the superior rectus muscle and the roof of the orbit, and may be difficult to separate from the superior rectus. The rectus muscles separate the intraconal space from the extraconal space. The lacrimal gland is located superolaterally in the orbit, with its vascular supply being the lacrimal artery. Tears produced by the lacrimal gland pass across the cornea and are absorbed through the lacrimal canaliculi of the upper and lower lids. In regard to innervation, CN III supplies the superior, inferior, and medial recti; the inferior oblique; and the levator palpebrae superioris muscles. CN IV supplies the superior oblique muscle and CN VI the lateral rectus muscle.
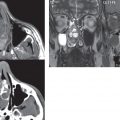
Evaluation of the orbit by CT includes reformatted thin sections in all three primary planes, with intravenous contrast necessary for soft tissue evaluation and assessment of lesion vascularity. MR scans are also typically obtained in all three planes, with fat suppression essential for evaluation of orbital contents and the optic nerve. Intravenous contrast is routinely employed, in particular, for evaluation of mass lesions and the optic nerve.
A few basic definitions are in order, in regard to orbital anomalies. In hypertelorism, the eyes (orbits) are farther apart than normal and, in hypotelorism, the eyes are abnormally too close. Exophthalmos (proptosis) is abnormal anterior protrusion of the globe.
Inflammation/Infection
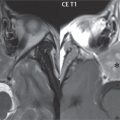
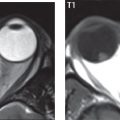
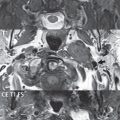
Orbital inflammation includes a number of diverse entities. Orbital cellulitis is divided into pre-septal and post-septal (orbital) types. In pre-septal cellulitis, infection is limited to the skin and subcutaneous tissues ( Fig. 2.34 ). In post-septal cellulitis inflammation involves the orbital contents. In the textbooks, it is stated that most orbital cellulitis is secondary to paranasal sinus infection (most commonly from the adjacent ethmoid sinuses). Spread from sinus infection can result in a subperiosteal or orbital abscess ( Fig. 2.35 ). This is usually treated as a surgical emergency. Cystic fibrosis is a predisposing condition. In severe cases of an orbital abscess there can be thrombosis of the ophthalmic veins and cavernous sinus. The term orbital pseudotumor refers to idiopathic orbital inflammation and is a diagnosis of exclusion. This entity is divided into subtypes, specifically anterior orbital inflammation, diffuse orbital pseudotumor, and orbital myositis ( Fig. 2.36 ).



In the anterior subtype, inflammation predominately involves the anterior orbit and globe. In the myositis sub-type, one or more of the extraocular muscles is primarily infiltrated and the tendons are typically involved. The differential diagnosis for the myositis subtype is thyroid orbitopathy. In thyroid associated orbitopathy, involvement of extraocular muscles is usually bilateral and symmetric (with accompanying exophthalmos). The most commonly involved muscles (in order of decreasing frequency) are the inferior, medial, superior, lateral, and oblique muscles (I′M SLO mnemonic). The enlargement of the muscles involves principally the bellies, sparing the tendons ( Fig. 2.37 ). On CT there may be heterogeneous areas of lower density within the muscles. On MR typical findings include muscle edema in the acute phase and prominent enhancement of the involved muscles.

Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


