This article addresses the imaging considerations for subtle early studies of imaging findings in sinusitis, focusing on early detection by the radiologist, which depend on dedicated imaging protocols and a careful, thorough search pattern. Pathogenesis and key imaging findings for orbital complications are discussed, followed by the intracranial complications of sinusitis.
Rhinosinusitis: complications in a common condition
Rhinosinusitis is a relatively common clinical condition affecting both children and adults. It is typically readily treated with nasal decongestants, with or without oral antibiotics. Rarely, sinus infection can result in vision loss or even life-threatening orbital and intracranial complications. Orbital extension of acute infection most commonly occurs in pediatric patients who typically present with proptosis, periorbital swelling, and erythema. When found in immunocompromised patients, such as those with diabetes, lymphoreticular malignancies, human immunodeficiency virus infection, chronic renal failure, or liver failure, intracranial infection is more likely to be secondary to acute invasive fungal sinusitis. However, orbital and/or intracranial complications may also occur in immunocompetent children, teenagers, and adults who are untreated or incompletely treated for bacterial rhinosinusitis. Although the consequences of sinogenic infections can be catastrophic, the imaging findings may be extremely subtle. Early detection of orbital and intracranial complications by the radiologist requires dedicated imaging protocols, knowledge of key imaging findings, and an understanding of disease pathogenesis.
Imaging considerations
Although radiographs may still be used to confirm the clinical impression of sinusitis, computed tomography (CT) is more accurate for making this diagnosis. Indeed, whenever orbital or intracranial complications of sinusitis are suspected, contrast-enhanced CT should be the initial imaging modality of choice. In the current era of more actively minimizing radiation exposure, particularly for pediatric patients, it is imperative that the study be performed with the lowest radiation dose possible, although this must not be at the expense of a diagnostic study. Sinogenic complications, especially in children and immunocompromised patients, may rapidly progress. It is imperative that referring clinicians indicate their concern for complications or clinical features that might suggest orbital or intracranial infection so that the scan protocol is correct.
Most of the published reports evaluating the role of CT for diagnosing orbital complications of sinusitis were based on CT imaging with what is now outdated technology. In addition to technologic constraints, such as slower acquisition times, decreased resolution, and nonvolumetric imaging, another limitation included the lag time between performing the CT and subsequent progression of symptoms in many of the reported cases. Despite these limitations, CT was still found to improve diagnostic accuracy relative to clinical judgment alone, a conclusion that certainly remains true today with improved CT technology.
With the continuous advancement of imaging, there are no prospective studies comparing current generation multidetector CT scanners with magnetic resonance (MR) imaging for the detection of orbital complications of sinusitis. McIntosh and Mahadevan recently reported the benefit of MR imaging over CT, but the MR imaging in their case report was performed after a delay during which the patient’s subperiosteal abscess likely progressed, as the abscess depicted with MR imaging would almost certainly have been visible with CT had it been performed simultaneously. Nevertheless, if follow-up imaging is deemed necessary to assess clinical deterioration or treatment response, MR imaging should be considered to spare the patient additional radiation exposure.
In evaluating the orbits, contrast-enhanced helical CT is best acquired in the axial plane using submillimeter collimation for isotropic voxels to allow for high-quality image reconstruction in the coronal and sagittal planes. Image data should be rendered using both soft tissue and bone algorithms to optimally assess the orbital contents as well as the thin osseous structures in the orbital and sinonasal regions. This multiplanar approach allows for more effective detection and localization of intraorbital pathology (particularly thin subperiosteal collections along the orbital roof or floor, which are more easily overlooked in the axial plane) and simultaneously provides a high-quality sinus CT that is equally necessary in this clinical context. With increased public awareness of iatrogenic radiation exposure, CT vendors are now offering radiation reduction options that include active dose modulation and improved iterative reconstruction techniques, both of which can maintain image quality while reducing dose. Although we typically use bismuth shielding to the orbits for head CT scans, this is not used at our institution for sinus CT studies because it prevents the use of the CT scan as an intraoperative stereotactic guide, and the patient would require additional scanning and thus further radiation.
Orbital MR imaging seems to be more sensitive for the detection of fungal sinusitis, with or without orbital or intracranial complications. In performing orbital MR imaging, specific imaging parameters vary based on equipment manufacturer and field strength. In general, axial and coronal T1-weighted sequences best depict the relevant orbital anatomy, and any infiltration or stranding of the normal high-intensity orbital fat should be sought as a sign of inflammation. A short tau inversion recovery (STIR) or T2-weighted fat-suppressed series should be included to evaluate for inflammatory edema and focal purulent fluid collections. Multiplanar postcontrast T1-weighted sequences with fat suppression should be acquired to search for inflammatory enhancement, as well as rim-enhancement patterns that may distinguish phlegmon from abscess. Although the local magnetic field is frequently inhomogeneous from dental hardware and air-bone interfaces in the face, it is helpful to carefully evaluate these fat-suppressed sequences in more than one plane to help distinguish high signal from failure of fat suppression versus true abnormal enhancement. In addition, the field of view for orbital MR imaging readily includes the parasellar region so the cavernous sinus should be assessed for thrombosis.
For suspected intracranial complications of sinusitis, contrast-enhanced head CT is useful as an initial screening test. Despite its limitations, CT can readily identify features that would immediately triage the patient for neurosurgical management such as significant mass effect, space-occupying brain lesions, large extraaxial collections, and hydrocephalus. Once contraindications have been ruled out, lumbar puncture can be safely performed to evaluate for meningitis while the patient awaits MR imaging to evaluate the intracranial contents with greater sensitivity and specificity than can be achieved with CT. The usefulness of different MR imaging pulse sequences is illustrated in greater detail through examples of specific intracranial complications.
Imaging considerations
Although radiographs may still be used to confirm the clinical impression of sinusitis, computed tomography (CT) is more accurate for making this diagnosis. Indeed, whenever orbital or intracranial complications of sinusitis are suspected, contrast-enhanced CT should be the initial imaging modality of choice. In the current era of more actively minimizing radiation exposure, particularly for pediatric patients, it is imperative that the study be performed with the lowest radiation dose possible, although this must not be at the expense of a diagnostic study. Sinogenic complications, especially in children and immunocompromised patients, may rapidly progress. It is imperative that referring clinicians indicate their concern for complications or clinical features that might suggest orbital or intracranial infection so that the scan protocol is correct.
Most of the published reports evaluating the role of CT for diagnosing orbital complications of sinusitis were based on CT imaging with what is now outdated technology. In addition to technologic constraints, such as slower acquisition times, decreased resolution, and nonvolumetric imaging, another limitation included the lag time between performing the CT and subsequent progression of symptoms in many of the reported cases. Despite these limitations, CT was still found to improve diagnostic accuracy relative to clinical judgment alone, a conclusion that certainly remains true today with improved CT technology.
With the continuous advancement of imaging, there are no prospective studies comparing current generation multidetector CT scanners with magnetic resonance (MR) imaging for the detection of orbital complications of sinusitis. McIntosh and Mahadevan recently reported the benefit of MR imaging over CT, but the MR imaging in their case report was performed after a delay during which the patient’s subperiosteal abscess likely progressed, as the abscess depicted with MR imaging would almost certainly have been visible with CT had it been performed simultaneously. Nevertheless, if follow-up imaging is deemed necessary to assess clinical deterioration or treatment response, MR imaging should be considered to spare the patient additional radiation exposure.
In evaluating the orbits, contrast-enhanced helical CT is best acquired in the axial plane using submillimeter collimation for isotropic voxels to allow for high-quality image reconstruction in the coronal and sagittal planes. Image data should be rendered using both soft tissue and bone algorithms to optimally assess the orbital contents as well as the thin osseous structures in the orbital and sinonasal regions. This multiplanar approach allows for more effective detection and localization of intraorbital pathology (particularly thin subperiosteal collections along the orbital roof or floor, which are more easily overlooked in the axial plane) and simultaneously provides a high-quality sinus CT that is equally necessary in this clinical context. With increased public awareness of iatrogenic radiation exposure, CT vendors are now offering radiation reduction options that include active dose modulation and improved iterative reconstruction techniques, both of which can maintain image quality while reducing dose. Although we typically use bismuth shielding to the orbits for head CT scans, this is not used at our institution for sinus CT studies because it prevents the use of the CT scan as an intraoperative stereotactic guide, and the patient would require additional scanning and thus further radiation.
Orbital MR imaging seems to be more sensitive for the detection of fungal sinusitis, with or without orbital or intracranial complications. In performing orbital MR imaging, specific imaging parameters vary based on equipment manufacturer and field strength. In general, axial and coronal T1-weighted sequences best depict the relevant orbital anatomy, and any infiltration or stranding of the normal high-intensity orbital fat should be sought as a sign of inflammation. A short tau inversion recovery (STIR) or T2-weighted fat-suppressed series should be included to evaluate for inflammatory edema and focal purulent fluid collections. Multiplanar postcontrast T1-weighted sequences with fat suppression should be acquired to search for inflammatory enhancement, as well as rim-enhancement patterns that may distinguish phlegmon from abscess. Although the local magnetic field is frequently inhomogeneous from dental hardware and air-bone interfaces in the face, it is helpful to carefully evaluate these fat-suppressed sequences in more than one plane to help distinguish high signal from failure of fat suppression versus true abnormal enhancement. In addition, the field of view for orbital MR imaging readily includes the parasellar region so the cavernous sinus should be assessed for thrombosis.
For suspected intracranial complications of sinusitis, contrast-enhanced head CT is useful as an initial screening test. Despite its limitations, CT can readily identify features that would immediately triage the patient for neurosurgical management such as significant mass effect, space-occupying brain lesions, large extraaxial collections, and hydrocephalus. Once contraindications have been ruled out, lumbar puncture can be safely performed to evaluate for meningitis while the patient awaits MR imaging to evaluate the intracranial contents with greater sensitivity and specificity than can be achieved with CT. The usefulness of different MR imaging pulse sequences is illustrated in greater detail through examples of specific intracranial complications.
Orbital complications of rhinosinusitis
Epidemiology and Pathogenesis of Orbital Spread of Infection
Largely because of proximity, orbital infection is the most common complication from acute sinusitis. Because the frontal and sphenoid sinuses develop at a later age, it is not surprising that involvement of the ethmoid sinuses is seen most often, followed in frequency by the maxillary sinuses. Because of anatomic, immunologic, and environmental factors, pediatric patients suffer from acute rhinosinusitis more frequently than adults, and account for the greater proportion of complicated cases. Recent series suggest that the average age of children with orbital complications is 6 to 8 years, although the median age tends to be slightly younger. Acute and chronic sinus disease, likewise, accounts for most cases of orbital cellulitis in adults, in whom there is a trend toward declining frequency with advancing age. Sinusitis-related orbital infection is the most common cause of unilateral proptosis in children and the third most common cause in adults after thyroid orbitopathy and pseudotumor. For unclear reasons, a male predominance is universally reported.
From an anatomic perspective, there are many predisposing factors that allow for spread of paranasal sinus infection to the orbit. In terms of physical proximity, the thin bony roof, floor, and medial wall of the orbit serve to separate the orbital contents from the frontal, maxillary, and ethmoid sinuses, respectively. Clearly, aggressive infections causing osteitis might directly extend from the sinus to the orbit, but this is rare and there are multiple other potential routes for the spread of infection that do not require transgression of intact bone. The orbit is formed from 7 separate bones, and this is most relevant in considering the medial wall, which is comprised of a small portion of the sphenoid body, the ethmoid lamina papyracea, the lacrimal bone, and the frontal process of the maxilla. The union of these bones results in the presence of 3 vertical sutures appropriately termed the sphenoethmoidal, lacrimoethmoidal, and lacrimomaxillary fissures. In addition, the anterior and posterior ethmoidal foramina allow transmission of vessels and nerves along the frontoethmoidal suture line. Focal osseous defects in the orbital walls can occur secondary to areas of congenital or acquired dehiscence, with the latter including sequela from both trauma and surgery.
The veins of the orbit also play a significant role in the pathogenesis of sinusitis-related complications, as it is a valveless system that allows 2-way communication between the veins of the face, paranasal sinuses, nasal cavity, orbit, pterygoid plexus, and cavernous sinus. The dominant venous drainage of the orbit is via the superior and inferior ophthalmic veins, although there are numerous smaller vessels forming a rich venous network. Most orbital and intracranial complications of sinusitis are secondary to transmission of infection via retrograde thrombophlebitis.
Despite the aforementioned features that predispose the spread of infection from the sinus to the orbit, a protective barrier exists in the form of the periorbita (ie, the periosteum of the orbit), which is analogous to the layer of dura lining the inner table of the calvarium. The periorbita is a robust fibrous membrane that can be stripped from the bone except at suture lines where it is contiguous with the periosteum on the other side. It not only serves as a barrier to the spread of infection from the sinuses to the orbit but also forms the anterior orbital septum as it reflects into the tarsal plates anteriorly. This creates a delineation between periorbital (preseptal) and intraorbital (postseptal) tissues, shielding the orbital contents from potential pathology.
Pathology and Imaging Detection
Chandler and colleagues eloquently described the role of the orbital anatomic structures in complications of sinusitis 4 decades ago. This formed the basis for their revised classification system that consists of the following groups:
- 1.
Inflammatory edema
- 2.
Orbital cellulitis
- 3.
Subperiosteal abscess
- 4.
Orbital abscess
- 5.
Cavernous sinus thrombosis.
Although still used today, there have been suggested modifications with the advent of cross-sectional imaging.
Inflammatory edema/preseptal cellulitis
Initially, the description of inflammatory edema referred to local inflammation and impaired venous drainage of the eyelids caused by increased pressure in ethmoid air cells, with or without edema of the orbits. Other investigators have subsequently revised this patient group to include those who have preseptal infection, defined as periorbital cellulitis with or without a focal abscess. The patient typically presents with eyelid erythema, tenderness, and swelling, and a detailed ophthalmologic examination is needed to ensure that underlying vision and extraocular motion is intact. Although isolated preseptal involvement frequently does not require cross-sectional imaging, it is useful when there is concern about postseptal extension.
On CT and MR imaging, infiltration of adipose tissue is seen in all types of edema, independent of whether it is a sterile hydrostatic process or frank cellulitis. Both modalities show swelling of the eyelids along with thickening and stranding of the periorbital soft tissues in cases of cellulitis, and the radiologist should evaluate for the development of a focal fluid collection to suggest an abscess ( Fig. 1 ). It is imperative to scrutinize the orbits to ensure that no postseptal involvement is present. The presence and extent of sinusitis should also be documented.
Preseptal cellulitis in children is less often associated with acute sinusitis than in adult patients, and is seen with greater frequency in the context of trauma (especially with a retained foreign body, laceration, or insect bite) and medical comorbidities.
Orbital cellulitis/postseptal cellulitis
Orbital cellulitis refers to postseptal edema involving the intra- and/or extraconal orbital contents. Although not a circumscribed process, the inflammation can be widespread or preferentially distributed in a certain portion of the orbit, in which it tends to be located adjacent to the most severely affected sinus. Depending on the amount of inflammation, varying degrees of proptosis and impairment of the function of extraocular muscles can occur. Orbital inflammation is well demonstrated with CT and appears as stranding of the orbital fat. The corresponding MR imaging appearance of this inflammatory infiltration is one of ill-defined T2 hyperintensity consistent with edema as well as concomitant enhancement following contrast administration ( Fig. 2 ).
Subperiosteal abscess
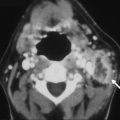
The subperiosteal abscess typically develops when ethmoid sinus infection spreads across the medial orbital wall or, less commonly, from the frontal or maxillary sinuses across the orbital roof or floor, respectively. The tough periorbita again serves as a barrier to free dissemination of infection throughout the orbital soft tissues; however, localized infection may evolve into an abscess that strips periorbita from bone, and displaces it inward. Typically, a thin fat plane is visible between the periorbita and the adjacent extraocular muscle. When small, a subperiosteal abscess causes minimal mass effect within the orbit and is seen as a subtle elongated rim-enhancing fluid collection ( Fig. 3 ). Larger subperiosteal abscesses assume a lenticular shape, exert significant mass effect, and can significantly impair extraocular motion and cause proptosis with compression and/or tethering of the optic nerve, resulting in vision loss ( Fig. 4 ). Coronal reformatted images of axial-acquired contrast-enhanced CT data should always be performed to evaluate for these collections, particularly if no cause for proptosis is evident on axial imaging. Indeed, a subperiosteal abscess arising from a frontal or maxillary sinus is most often readily identified in the coronal (or sagittal) plane.
Orbital abscess
Whether intra- or extraconal, an orbital abscess is a collection of pus that is not contained by the periorbita. Orbital abscesses usually cause proptosis, ophthalmoplegia, and visual impairment, and these clinical signs are more marked with larger abscesses or orbital apex involvement. Mass effect within the more tightly confined orbital apex is more apt to involve cranial nerves II, III, IV, and VI, as well as the ophthalmic branch of cranial nerve V, because these structures exit the optic foramen and superior orbital fissure. Unlike the poorly defined edema and enhancement seen with orbital cellulitis, an orbital abscess is seen as a more discrete rim-enhancing fluid collection within the orbital adipose tissue with extensive surrounding inflammation ( Fig. 5 ).
Cavernous sinus thrombosis
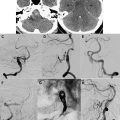
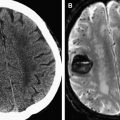
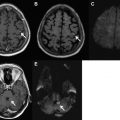
Many cases of cavernous sinus thrombosis associated with rhinosinusitis are clinically apparent. Patients typically present with fever, headache, periorbital swelling, diplopia, chemosis, and/or proptosis. Sixth nerve palsy is most commonly seen, but additional involvement of the third, fourth, fifth, or sixth cranial nerves in the context of orbital or sinus infection should heighten concern for cavernous sinus thrombosis. Contrast-enhanced CT may be unrevealing initially, but fulminate cases show a heterogeneous pattern of less than expected enhancement of the cavernous sinus, which makes the cavernous segment of the internal carotid artery more conspicuous. In addition, the cavernous sinus becomes thickened and the lateral margin assumes a convex morphology. An area of nonopacification exceeding 7 mm in maximum dimension is more common in cases of cavernous sinus thrombosis than in control patients, and this is even more suggestive when present posteriorly. Indirect venous findings, which can be helpful in directing attention to the cavernous sinus, include filling defects or expansion of the superior ophthalmic vein, the inferior petrosal sinus, and sphenoparietal sinus. A similar pattern of abnormality is seen with MR imaging using a contrast-enhanced T1-weighted sequence, with the lateral convexity best demonstrated in the coronal plane ( Fig. 6 ). Increased dural enhancement along the lateral border of the cavernous sinus on MR imaging represents an additional indirect finding. Inflammation within the cavernous sinus can lead to narrowing or occlusion of the ipsilateral internal carotid artery, which may result in acute cerebral infarction.
Thrombosis of the superior or inferior ophthalmic veins secondary to sinus infection may be seen as a precursor to, or as a result of, cavernous sinus thrombosis. In addition to the expected distension and incomplete enhancement of the ophthalmic veins in these patients, restricted diffusion may provide a clue to this diagnosis as well ( Fig. 7 ). In cases of fulminate thrombophlebitis, it is difficult to delineate whether these diffusion characteristics are secondary to the stage of intravenous blood degradation or the purulent nature of the venous contents.
Related posts:
 Acute Neurointerventional Therapies
Acute Neurointerventional Therapies
 Intracranial Hypotension and Intracranial Hypertension
Seizures: Emergency Neuroimaging
Intracranial Hypotension and Intracranial Hypertension
Seizures: Emergency Neuroimaging
 Nontraumatic Intracranial Hemorrhage
Nontraumatic Intracranial Hemorrhage
 Emergency Head & Neck Imaging: Infections and Inflammatory Processes
Emergency Head & Neck Imaging: Infections and Inflammatory Processes
 Diffusion MR Imaging: An Important Tool in the Assessment of Brain Tumors
Diffusion MR Imaging: An Important Tool in the Assessment of Brain Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


