Presentation and Presenting Images
A 35-year-old female whose mother and grandmother had premenopausal breast cancer presents for high-risk screening mammography.
17.2 Key images
( ▶ Fig. 17.3, ▶ Fig. 17.4, ▶ Fig. 17.5, ▶ Fig. 17.6, ▶ Fig. 17.7, ▶ Fig. 17.8)
17.2.1 Breast Tissue Density
The breasts are heterogeneously dense, which may obscure small masses.
17.2.2 Imaging Findings
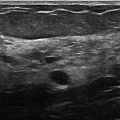
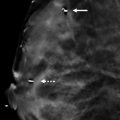
Superficially within the upper outer quadrant of the right breast, there is an oval circumscribed mass that is best seen on the craniocaudal (CC) view ( ▶ Fig. 17.3), and is obscured on the mediolateral oblique (MLO) view ( ▶ Fig. 17.4). The digital breast tomosynthesis (DBT) images are helpful to isolate this mass from the surrounding tissues ( ▶ Fig. 17.5 and ▶ Fig. 17.6). On the CC DBT image, there is a suggestion of a fatty cleft ( ▶ Fig. 17.5). Historical magnetic resonance images (MRI) from the patient demonstrate the classic appearance of a lymph node. The mass is isointense to the glandular tissue on the T1-weighted MRI with a cleft that is the same as the signal intensity of fat ( ▶ Fig. 17.7). On the T2-wieghted MRI, the mass has increased signal intensity with a central cleft that has decreased signal intensity similar to the surrounding fatty tissue ( ▶ Fig. 17.8).
17.3 BI-RADS Classification and Action
Category 2: Benign
17.4 Differential Diagnosis
Lymph node: This mass is circumscribed and contains a fatty hilum, which is supported by the DBT images. Additionally, historical MR images demonstrate the classic appearance of a superficially located lymph node in the upper outer quadrant of the breast.
Fibroadenoma: Fibroadenomas can occur anywhere in the breast and are very common in patients this age. They can share common characteristics of a lymph node on MR imaging. The presence of a fatty hilum makes a fibroadenoma a less likely diagnosis.
Cyst: Cysts can have variable appearances. The historical MR imaging favors a lymph node over a cyst.
17.5 Essential Facts
DBT may help in averting a recall mammogram or a biopsy by better defining a lesion seen on full-field digital mammography (FFDM). In this case, the CC FFDM suggested a lymph node. The MLO view was not helpful. The DBT images were helpful in defining this mass as a lymph node even before exploring the historical MR imaging.
DBT can be helpful to assess for the presence of a fatty hilum not only in intramammary nodes, but also in axillary nodes. The axilla should be part of the normal search pattern.
Recall rates have been shown to be significantly decreased with DBT without sacrificing sensitivity.
Studies have reported that DBT also reduces the false-positive recalls by 40%.
17.6 Management and Digital Breast Tomosynthesis Principles
It is important to use all historical imaging studies available when evaluating findings at screening mammography. Finding a CT or MR image that can help confirm FFDM or DBT findings helps reduce unnecessary recalls. The electronic medical record (EMR) and picture archiving and communication systems (PACs) have allowed more access to a patient’s additional nonbreast imaging studies.
Some benign-appearing lesions will only be seen on DBT. This is especially reported in dense fibroglandular tissue. A metric needs to be established to know which of these can be dismissed and which may need further evaluation.
17.7 Further Reading
[1] Baker JA, Lo JY. Breast tomosynthesis: state-of-the-art and review of the literature. Acad Radiol. 2011; 18(10): 1298‐1310 PubMed
[2] Conant EF. Clinical implementation of digital breast tomosynthesis. Radiol Clin North Am. 2014; 52(3): 499‐518 PubMed

Fig. 17.1 Right craniocaudal (RCC) mammogram.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


