• A rare lesion caused by hamartomatous proliferation of the terminal bronchioles at the expense of alveolar development • It is usually unilobar and communicates with a normal tracheobronchial tree • A congenital mass of aberrant pulmonary tissue that has no normal connection with the bronchial tree or pulmonary arteries • It derives its arterial supply from either the thoracic or abdominal aorta • A congenital marked over-aeration of a single pulmonary lobe (usually an upper lobe and less commonly the middle lobe) • It results from bronchial obstruction by a ‘ball-valve’ mechanism of unknown aetiology
Paediatric chest
CONGENITAL CHEST ABNORMALITIES
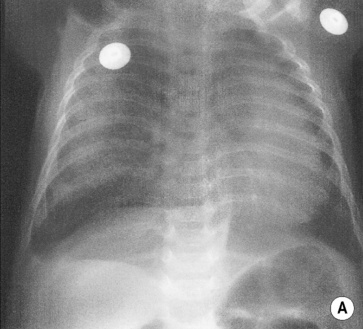
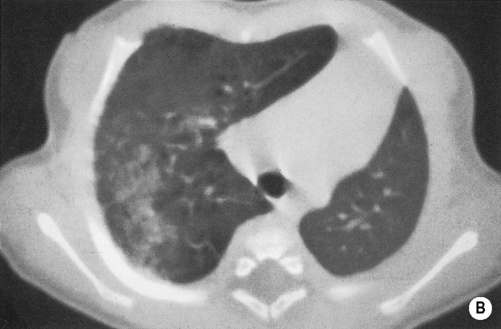
CONGENITAL CYSTIC ADENOMATOID MALFORMATION
DEFINITION
 it is characterized by a multicystic mass of pulmonary tissue with proliferation of the bronchiolar structures
it is characterized by a multicystic mass of pulmonary tissue with proliferation of the bronchiolar structures
 it receives its blood supply from a normal pulmonary artery and vein
it receives its blood supply from a normal pulmonary artery and vein  it may compress the contralateral lung (resulting in hypoplasia)
it may compress the contralateral lung (resulting in hypoplasia)
CONGENITAL CHEST ABNORMALITIES
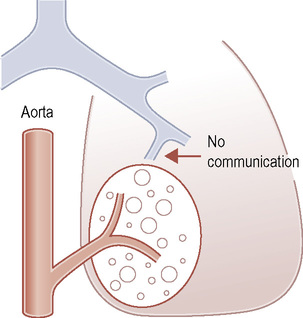
BRONCHOPULMONARY SEQUESTRATION
DEFINITION
 lesions are defined as either intra- or extralobar
lesions are defined as either intra- or extralobar
 its venous drainage can either be via the pulmonary or systemic veins
its venous drainage can either be via the pulmonary or systemic veins
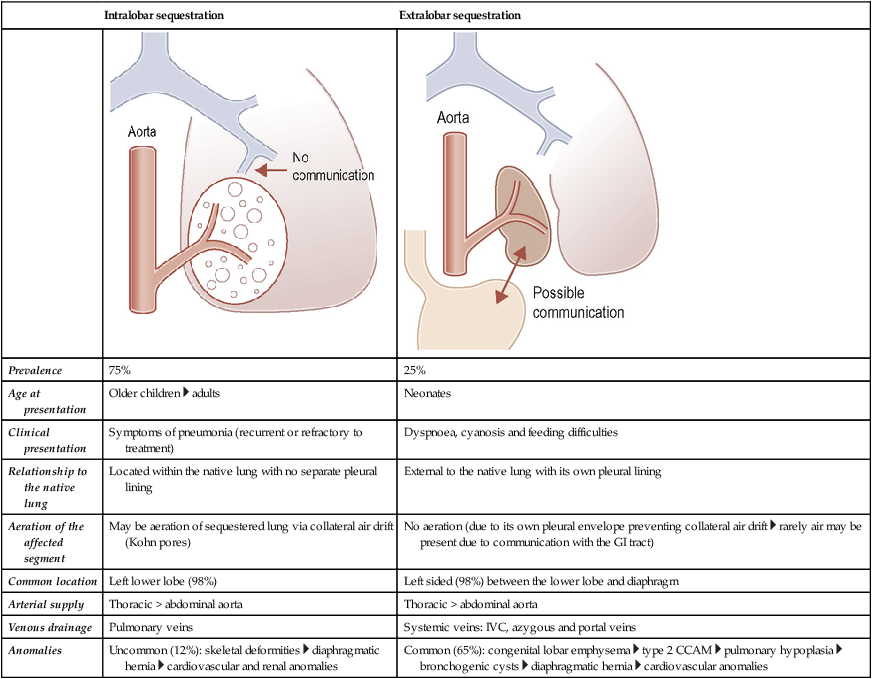
Intralobar sequestration
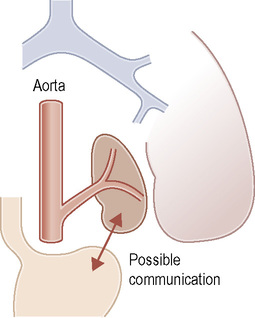
Extralobar sequestration
Prevalence
75%
25%
Age at presentation
Older children  adults
adults
Neonates
Clinical presentation
Symptoms of pneumonia (recurrent or refractory to treatment)
Dyspnoea, cyanosis and feeding difficulties
Relationship to the native lung
Located within the native lung with no separate pleural lining
External to the native lung with its own pleural lining
Aeration of the affected segment
May be aeration of sequestered lung via collateral air drift (Kohn pores)
No aeration (due to its own pleural envelope preventing collateral air drift  rarely air may be present due to communication with the GI tract)
rarely air may be present due to communication with the GI tract)
Common location
Left lower lobe (98%)
Left sided (98%) between the lower lobe and diaphragm
Arterial supply
Thoracic > abdominal aorta
Thoracic > abdominal aorta
Venous drainage
Pulmonary veins
Systemic veins: IVC, azygous and portal veins
Anomalies
Uncommon (12%): skeletal deformities  diaphragmatic hernia
diaphragmatic hernia  cardiovascular and renal anomalies
cardiovascular and renal anomalies
Common (65%): congenital lobar emphysema  type 2 CCAM
type 2 CCAM  pulmonary hypoplasia
pulmonary hypoplasia  bronchogenic cysts
bronchogenic cysts  diaphragmatic hernia
diaphragmatic hernia  cardiovascular anomalies
cardiovascular anomalies
CONGENITAL CHEST ABNORMALITIES
CONGENITAL LOBAR EMPHYSEMA
DEFINITION
 possible causes:
possible causes:Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Paediatric chest

 this has a good prognosis (and an infrequent association with other congenital abnormalities)
this has a good prognosis (and an infrequent association with other congenital abnormalities)
 congenital malformations are common (50%)
congenital malformations are common (50%)
 it has a poor prognosis due to the associated congenital malformations and severe respiratory compromise
it has a poor prognosis due to the associated congenital malformations and severe respiratory compromise symptoms are due to a combination of obstructive emphysema, mediastinal shift and infection
symptoms are due to a combination of obstructive emphysema, mediastinal shift and infection once this fluid has been reabsorbed it will be replaced by an air-filled cystic lesion
once this fluid has been reabsorbed it will be replaced by an air-filled cystic lesion



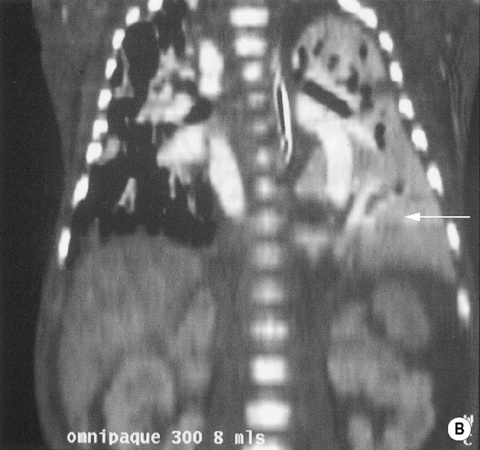
 the anomalous systemic arterial supply is difficult to visualize despite the availability of colour flow Doppler
the anomalous systemic arterial supply is difficult to visualize despite the availability of colour flow Doppler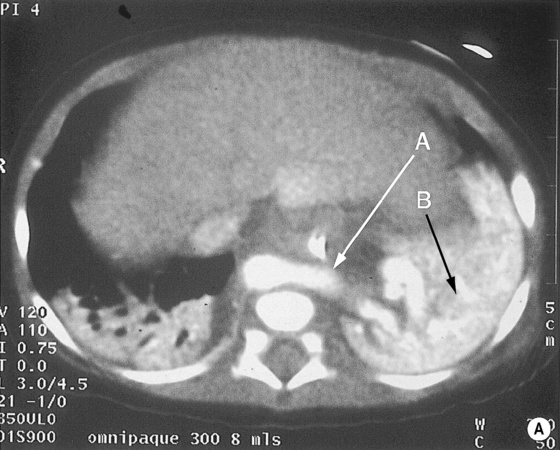
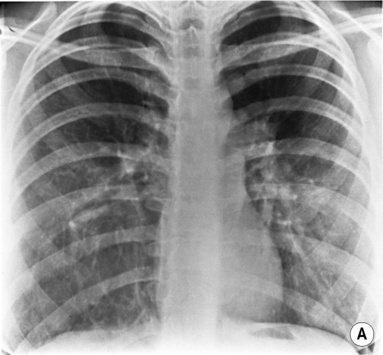
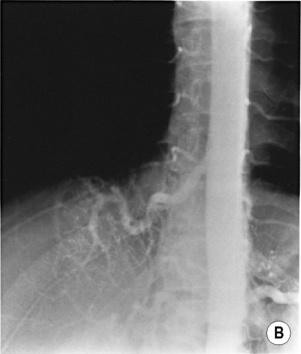
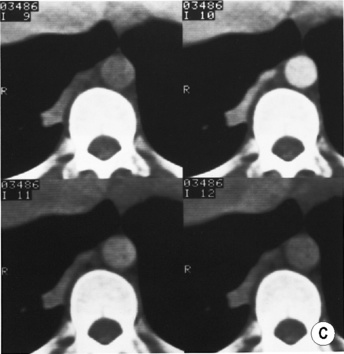
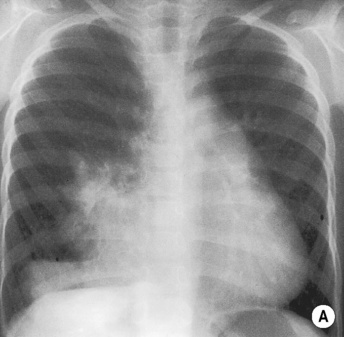
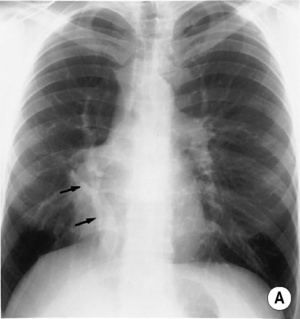
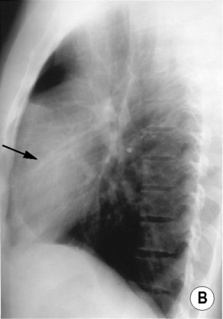
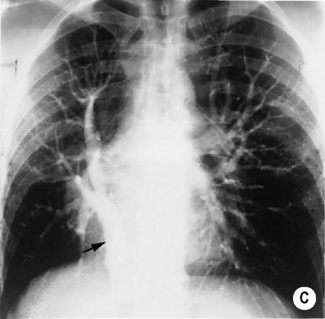
 this suggests they may be draped around a space-occupying but air-filled lesion. The right hemidiaphragm is slightly depressed and the heart is shifted slightly to the left. (B) Aortogram demonstrates a large single vessel arising from the distal aorta supplying a portion of the right lower lobe. (C) CECT confirms the vascular supply.
this suggests they may be draped around a space-occupying but air-filled lesion. The right hemidiaphragm is slightly depressed and the heart is shifted slightly to the left. (B) Aortogram demonstrates a large single vessel arising from the distal aorta supplying a portion of the right lower lobe. (C) CECT confirms the vascular supply.




