• The ascent of the fused kidney is arrested by the inferior mesenteric artery during development, resulting in a low abdominal position (the isthmus lies anterior to the aorta and IVC but posterior to the inferior mesenteric artery) • It is always associated with malrotation so that the pelves and ureters pass anteriorly over the fused lower poles • The upper pole of the kidney is located more laterally than the lower pole (the upper pole calyces are therefore lateral to the lower pole calyces) • Failure of complete ascent: this results in a pelvic kidney (the majority) • Overascent: this is almost always limited by the diaphragm but if there is eventration of the diaphragm or a Bochdalek hernia an intrathoracic kidney may result • This follows failure of the ureteric bud to reach the metanephros (affecting 1 in 1250 live births) • A congenital abnormality where drainage of the kidney is via two collecting systems (occurring in 3% of individuals) – The upper moiety ureter usually enters the bladder as a ureterocele • Asymptomatic • Pain: secondary to intermittent obstruction at the PUJ level of the lower moiety or due to ‘yo–yo’ reflux with incomplete duplication • Continuous wetting in a girl: due to an ectopic insertion of the upper moiety into the vagina • Vaginal prolapse: the ureterocele prolapses out of the bladder • Bladder neck obstruction: following prolapse of a ureterocele • Upper moiety: this may be normal, small, or dysplastic • Lower moiety: in complete duplication the lower moiety may be normal and difficult to recognize • Ureterocele: this is seen at the bladder base if it is intravesical • It may also prolapse into the urethra (causing bladder outlet obstruction) or present as a labial and interlabial mass • Ureteroceles that are not associated with a duplex system tend to be small and are not associated with significant obstruction (unless complicated by calculi) US A thin-walled cystic structure projecting into the bladder lumen • Medullary cysts associated with interstitial fibrosis and tubular atrophy
Paediatric genitourinary disorders
CONGENITAL RENAL ANOMALIES
ABNORMALITIES OF FUSION
DUPLEX KIDNEY
HORSESHOE KIDNEY
Definition
 its abnormal position makes it more susceptible to injury
its abnormal position makes it more susceptible to injury
ABNORMALITIES OF POSITION
MALROTATED KIDNEY
 a malrotated kidney may develop urological complications, be more susceptible to trauma, or indicate that pathology in an adjacent organ is displacing the kidney
a malrotated kidney may develop urological complications, be more susceptible to trauma, or indicate that pathology in an adjacent organ is displacing the kidney
ECTOPIC KIDNEY
 there is an increased risk of trauma, VUR and calculus formation (due to urinary stasis)
there is an increased risk of trauma, VUR and calculus formation (due to urinary stasis)
 this can resemble a posterior mediastinal mass
this can resemble a posterior mediastinal mass
CONGENITAL RENAL ANOMALIES
UNILATERAL RENAL AGENESIS
DEFINITION
 the ipsilateral ureter and hemitrigone fail to develop but occasionally a ureteric stump may remain
the ipsilateral ureter and hemitrigone fail to develop but occasionally a ureteric stump may remain  as an antenatal diagnosis is uncommon this suggests that agenesis may represent an involuted multicystic kidney
as an antenatal diagnosis is uncommon this suggests that agenesis may represent an involuted multicystic kidney  bilateral renal agenesis is incompatible with life
bilateral renal agenesis is incompatible with life
DUPLEX KIDNEY
DUPLEX KIDNEY
DEFINITION
 The ureters draining the two moieties never join
The ureters draining the two moieties never join
 such ectopic drainage is almost always associated with dysplastic function of the upper moiety of the kidney
such ectopic drainage is almost always associated with dysplastic function of the upper moiety of the kidney
CLINICAL PRESENTATION
 the development of a UTI
the development of a UTI
RADIOLOGICAL FEATURES
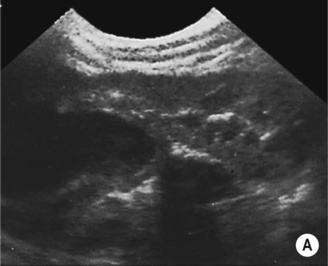
US
 it may be anechoic and resemble a ‘cyst’ (which is an obstructed ureterocele)
it may be anechoic and resemble a ‘cyst’ (which is an obstructed ureterocele)  these findings are generally associated with a dilated ureter
these findings are generally associated with a dilated ureter
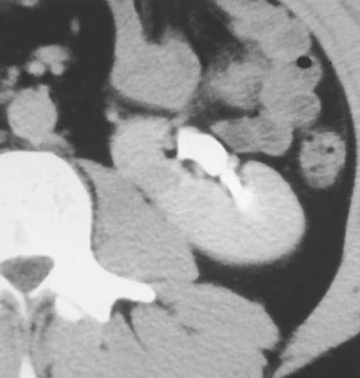
 the calyces and pelvis of a lower moiety may be dilated with no ureteric dilatation (suggesting a PUJ stenosis)
the calyces and pelvis of a lower moiety may be dilated with no ureteric dilatation (suggesting a PUJ stenosis)  reflux is likely when a dilated ureter is seen
reflux is likely when a dilated ureter is seen
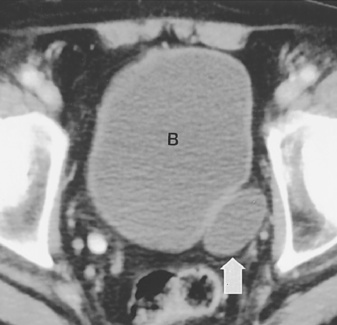
 it can be so large as to be mistaken for a bladder
it can be so large as to be mistaken for a bladder
PEARLS
Ureterocele
CONGENITAL RENAL CYSTIC DISEASE
JUVENILE NEPHRONOPHTHISIS/MEDULLARY CYSTIC DISEASE
DEFINITION
Paediatric genitourinary disorders
 the isthmus may be anything from a fibrous band, to more commonly a block of renal tissue
the isthmus may be anything from a fibrous band, to more commonly a block of renal tissue
 duplicated ureter (10%)
duplicated ureter (10%)  medullary sponge kidney
medullary sponge kidney  anorectal and musculoskeletal anomalies
anorectal and musculoskeletal anomalies
 renal calculi or infection
renal calculi or infection  there is an increased risk of renal tumours (e.g. a Wilms’ tumour)
there is an increased risk of renal tumours (e.g. a Wilms’ tumour) there is an increased incidence of VUR into the crossed kidney
there is an increased incidence of VUR into the crossed kidney it is more common on the right (M>F)
it is more common on the right (M>F)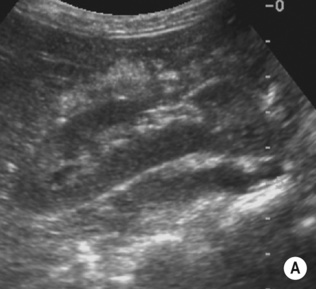







 cardiovascular, gastrointestinal and musculoskeletal anomalies
cardiovascular, gastrointestinal and musculoskeletal anomalies  the VATER syndrome
the VATER syndrome
 renal cysts or a renal carcinoma can also be present
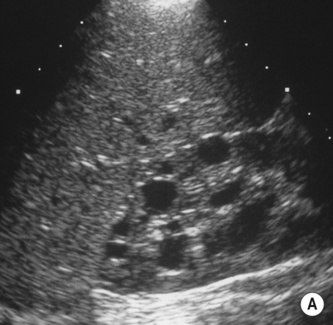
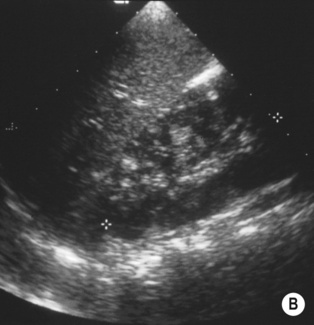
renal cysts or a renal carcinoma can also be present during later childhood there may be multiple small rounded echogenic foci throughout the renal parenchyma representing multiple AMLs (with an increased risk of haemorrhage if an AML is > 4cm)
during later childhood there may be multiple small rounded echogenic foci throughout the renal parenchyma representing multiple AMLs (with an increased risk of haemorrhage if an AML is > 4cm) it is usually left sided, hypoplastic and caudally positioned
it is usually left sided, hypoplastic and caudally positioned it is usually located at the junction of the upper and middle ⅓ of the kidney
it is usually located at the junction of the upper and middle ⅓ of the kidney  it may be mistaken for a renal mass and is associated with a bifid renal pelvis
it may be mistaken for a renal mass and is associated with a bifid renal pelvis it may be mistaken for a renal mass
it may be mistaken for a renal mass







 posterior urethra
posterior urethra  seminal vesicle or ejaculatory duct
seminal vesicle or ejaculatory duct  vagina
vagina


 the kidney may simply show two distinct renal pelves
the kidney may simply show two distinct renal pelves if a moiety is non-functional it will not be visualized (this is important to recognise when there is a small severely dysplastic upper moiety)
if a moiety is non-functional it will not be visualized (this is important to recognise when there is a small severely dysplastic upper moiety)  with incomplete duplication the upper and lower moieties may be normal or there may be reduced function of either element
with incomplete duplication the upper and lower moieties may be normal or there may be reduced function of either element reflux into the upper moiety is rarely detected
reflux into the upper moiety is rarely detected it is usually associated with the upper moiety ureter of a duplex system (and may obstruct the ipsilateral lower moiety ureter)
it is usually associated with the upper moiety ureter of a duplex system (and may obstruct the ipsilateral lower moiety ureter)




 a small amount of contrast medium is seen in the bladder but no ureterocele is evident.*
a small amount of contrast medium is seen in the bladder but no ureterocele is evident.*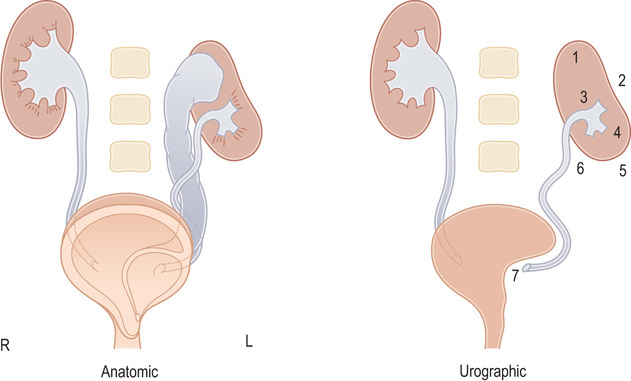
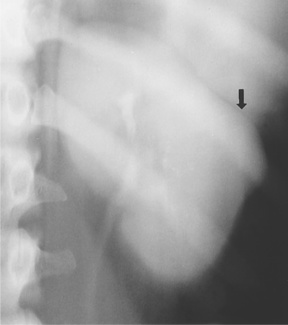
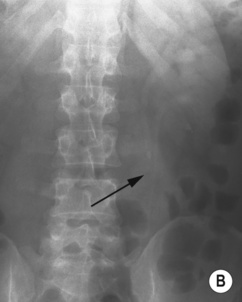
 2, abnormal axis of the collecting system
2, abnormal axis of the collecting system  3, impression upon the upper border of the renal pelvis
3, impression upon the upper border of the renal pelvis  4, decreased number of calyces compared to the contralateral kidney
4, decreased number of calyces compared to the contralateral kidney  5, lateral displacement of the kidney and ureter
5, lateral displacement of the kidney and ureter  6, lateral course of the visualized ureter
6, lateral course of the visualized ureter  7, filling defect in the bladder.
7, filling defect in the bladder.
 there is a prolonged course with an average disease duration of 10 years
there is a prolonged course with an average disease duration of 10 years







